Clinical question: In adults with acute pancreatitis, does early aggressive fluid resuscitation improve outcomes compared with a more moderate fluid strategy?
Acute pancreatitis is one of those conditions where “give fluids early” has been drilled into clinical practice for years. The logic makes sense: patients may be volume depleted, pancreatic microcirculation may be impaired, and early resuscitation could theoretically reduce ischemia, necrosis, and progression to severe disease.
But the key question has always been: how much fluid is too much?
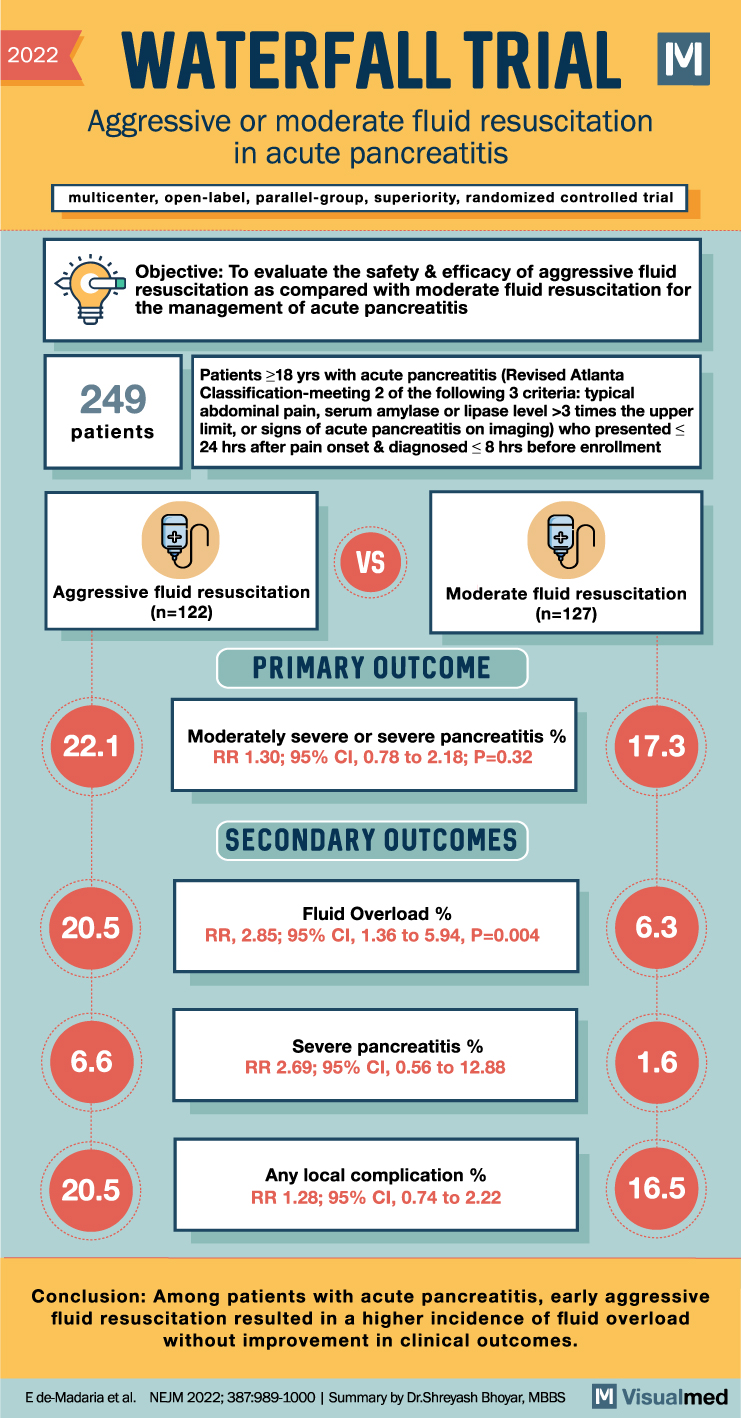
The WATERFALL trial directly addressed this question by comparing aggressive versus moderate lactated Ringer’s fluid resuscitation in patients presenting early with acute pancreatitis. The study was a multicenter, open-label, randomized controlled trial that enrolled adults with acute pancreatitis within 24 hours of pain onset and within 8 hours of diagnosis.
Study Design
The trial randomized 249 patients with acute pancreatitis:
Aggressive fluid resuscitation: 122 patients
Moderate fluid resuscitation: 127 patients
The aggressive strategy used a higher upfront bolus and higher maintenance infusion rate, whereas the moderate strategy used more selective bolusing and lower-rate hydration. Lactated Ringer’s solution was used in both groups. Patients were reassessed at prespecified time points for volume status, safety, and need for adjustment.
Importantly, this was not a trial of patients with established severe pancreatitis or shock at baseline. Patients with moderately severe or severe acute pancreatitis at presentation, significant heart failure, chronic renal failure, decompensated liver disease, and other high-risk comorbidities were excluded.
Primary Outcome
The primary outcome was development of moderately severe or severe acute pancreatitis.
Aggressive fluids did not improve the primary outcome:
22.1% with aggressive resuscitation
17.3% with moderate resuscitation
RR 1.30; 95% CI 0.78–2.18; P=0.32
So, despite receiving more fluid, patients in the aggressive group did not have better clinical outcomes. If anything, the point estimate numerically favored the moderate fluid group.
Safety Outcome: Fluid Overload
The most important signal from WATERFALL was harm.
Fluid overload occurred much more frequently with aggressive resuscitation:
20.5% with aggressive fluids
6.3% with moderate fluids
RR 2.85; 95% CI 1.36–5.94; P=0.004
The trial was stopped early because of worse safety outcomes in the aggressive-resuscitation group without a corresponding improvement in pancreatitis-related outcomes.
Secondary Outcomes
Secondary outcomes also did not show a meaningful benefit with aggressive fluids.
Severe pancreatitis occurred in:
6.6% with aggressive resuscitation
1.6% with moderate resuscitation
RR 2.69; 95% CI 0.56–12.88
Any local complication occurred in:
20.5% with aggressive resuscitation
16.5% with moderate resuscitation
RR 1.28; 95% CI 0.74–2.22
Overall, aggressive hydration increased fluid overload and did not reduce progression to more severe pancreatitis.
Clinical Interpretation
The WATERFALL trial changed the tone around fluid management in acute pancreatitis.
The message is not that patients with acute pancreatitis should be under-resuscitated. Early fluids still matter, especially when patients are hypovolemic. But WATERFALL argues strongly against a reflexive, one-size-fits-all aggressive fluid strategy in mild acute pancreatitis.
A better approach is:
Start with moderate hydration. Reassess frequently. Bolus selectively. Watch closely for fluid overload.
This is especially relevant because many patients with acute pancreatitis are older or have comorbid cardiac, renal, or pulmonary disease, where excess fluid can quickly cause harm.
Limitations
WATERFALL was open-label, stopped early, and enrolled a relatively lower-risk acute pancreatitis population. Patients with severe pancreatitis at baseline were excluded, so the results should not be automatically applied to patients presenting with shock, organ failure, or severe hypovolemia.
Still, for the typical hospitalized patient presenting early with mild acute pancreatitis, the trial provides strong evidence that more fluid is not necessarily better.
Bottom Line
In the WATERFALL trial, early aggressive fluid resuscitation in acute pancreatitis increased fluid overload without improving clinical outcomes.
For most patients with early acute pancreatitis, moderate lactated Ringer’s resuscitation with frequent reassessment appears safer than routine aggressive hydration.
Clinical takeaway:
Do not drown the pancreas. Resuscitate, reassess, and individualize.