Helicobacter pylori is one of the most important infections in gastroenterology. It commonly colonizes the gastric mucosa and may remain silent for years, but when clinically relevant, it is strongly linked with chronic active gastritis, peptic ulcer disease, upper GI bleeding, gastric adenocarcinoma, and gastric MALT lymphoma. Chronic infection can cause long-standing gastric inflammation and is associated with gastric adenocarcinoma and gastric mucosa-associated lymphoid tissue lymphoma.
Why H. pylori matters
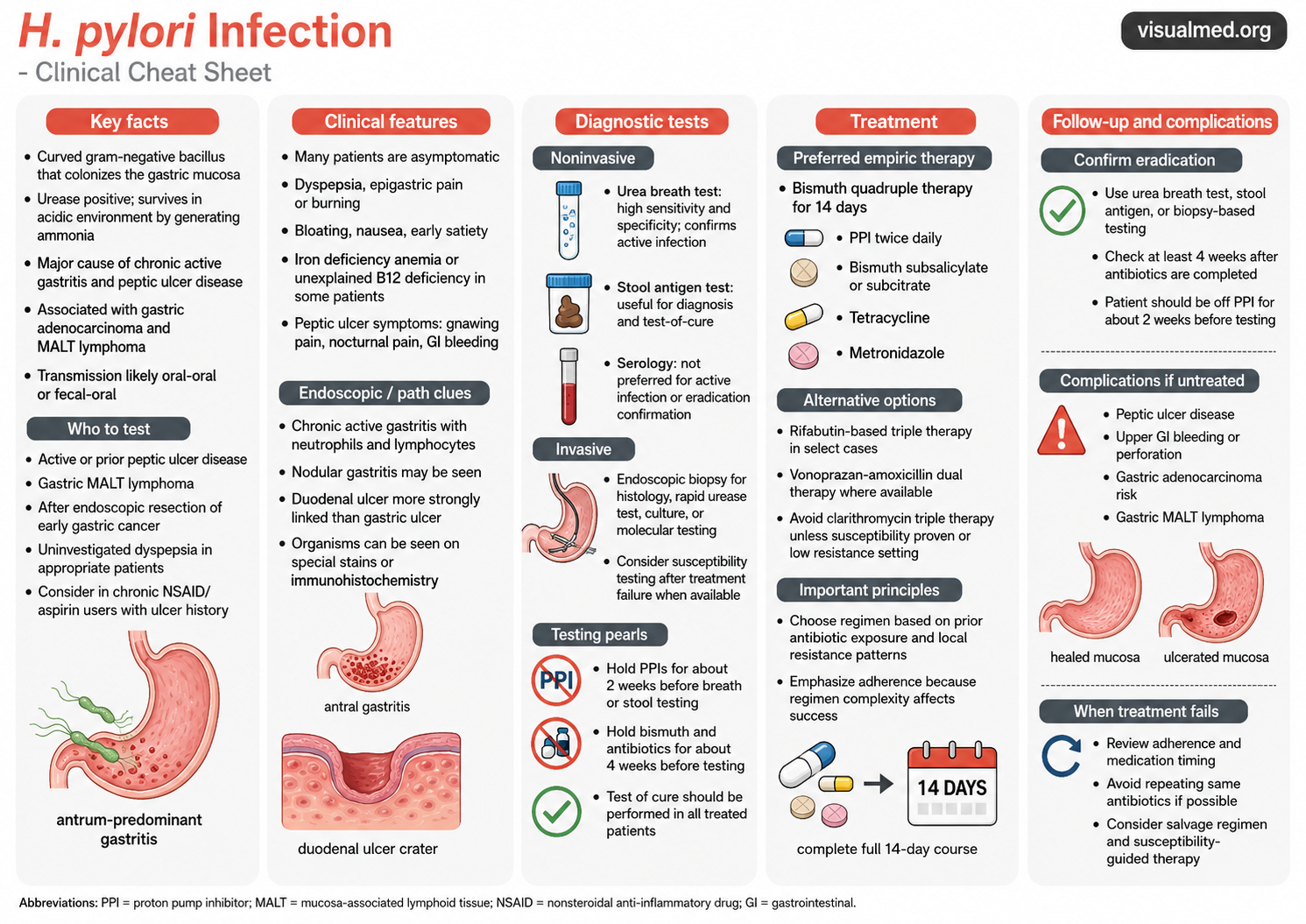
Most patients with H. pylori infection are asymptomatic. When symptoms occur, they often reflect gastritis or peptic ulcer disease and may include epigastric burning or aching pain, bloating, early satiety, nausea, reduced appetite, belching, or weight loss. Red flags such as melena, hematemesis, severe persistent abdominal pain, dysphagia, dizziness, or syncope require urgent evaluation.
The organism survives in the acidic stomach environment partly through urease activity, which helps neutralize local acidity and supports colonization of the gastric mucosa. Clinically, this makes H. pylori a high-yield diagnosis to remember in patients with dyspepsia, unexplained iron deficiency anemia, B12 deficiency, peptic ulcer symptoms, or a history of gastric MALT lymphoma or early gastric cancer.
Who should be tested?
Testing is most important when the result will change management. Common groups to test include patients with active or prior peptic ulcer disease, suspected or confirmed gastric MALT lymphoma, prior endoscopic resection of early gastric cancer, and appropriate patients with uninvestigated dyspepsia. The 2024 ACG update also highlights expanded testing considerations for patients at increased gastric cancer risk, those with atrophic gastritis or gastric intestinal metaplasia, and household members of adults with confirmed H. pylori infection using non-serologic testing.
Diagnostic testing: noninvasive first when appropriate
For most outpatient scenarios, the key noninvasive tests are the urea breath test and stool antigen test. Both can detect active infection and can also be used later to confirm eradication. Mayo Clinic describes stool antigen testing, urea breath testing, and endoscopic biopsy-based testing as diagnostic options, with endoscopy generally reserved for patients who need direct visualization, biopsy, evaluation of ulcer disease, alarm symptoms, or further workup.
Serology is less useful when active infection or eradication needs to be confirmed, because antibody tests may remain positive after prior exposure. In practice, breath testing, stool antigen testing, or biopsy-based testing is preferred when the clinical question is: “Does this patient currently have H. pylori?”
Treatment: 14 days matters
Current North American treatment has moved away from routine clarithromycin-based triple therapy because resistance has reduced efficacy. The 2024 ACG guideline recommends optimized bismuth quadruple therapy for 14 days as the preferred empiric regimen for treatment-naïve adults when susceptibility is unknown. This regimen includes a PPI twice daily, bismuth subsalicylate or subcitrate, tetracycline, and metronidazole.
Alternative suggested regimens include rifabutin-based triple therapy and vonoprazan-amoxicillin dual therapy where appropriate and available. The ACG specifically recommends avoiding empiric PPI-clarithromycin triple therapy unless susceptibility testing confirms clarithromycin sensitivity.
The practical point: adherence is everything. Bismuth quadruple therapy is effective, but it is complex. Patients need clear instructions, medication timing, side-effect counseling, and a plan to complete the full 14-day course.
Test-of-cure is not optional
Every treated patient should have eradication confirmed. The ACG emphasizes proof of eradication in all patients using fecal antigen testing, urea breath testing, or gastric biopsy. Testing should be delayed until at least 4 weeks after antibiotics are completed, and the patient should be off PPIs or PCABs for at least 2 weeks before testing to reduce false-negative results. Mayo Clinic similarly recommends follow-up testing at least four weeks after treatment.
What to do when treatment fails
If H. pylori persists, the first step is to review adherence, dosing, medication timing, and whether acid suppression or antibiotics were held appropriately before the test-of-cure. Avoid simply repeating the same antibiotic regimen if failure is likely due to resistance. Consider a salvage regimen based on prior antibiotic exposure, local resistance patterns, and susceptibility testing when available.
Clinical bottom line
H. pylori is common, often silent, and clinically important. The modern approach is straightforward: test the right patients, use active-infection testing, treat with an effective 14-day regimen, avoid empiric clarithromycin triple therapy unless susceptibility is known, and always confirm eradication.