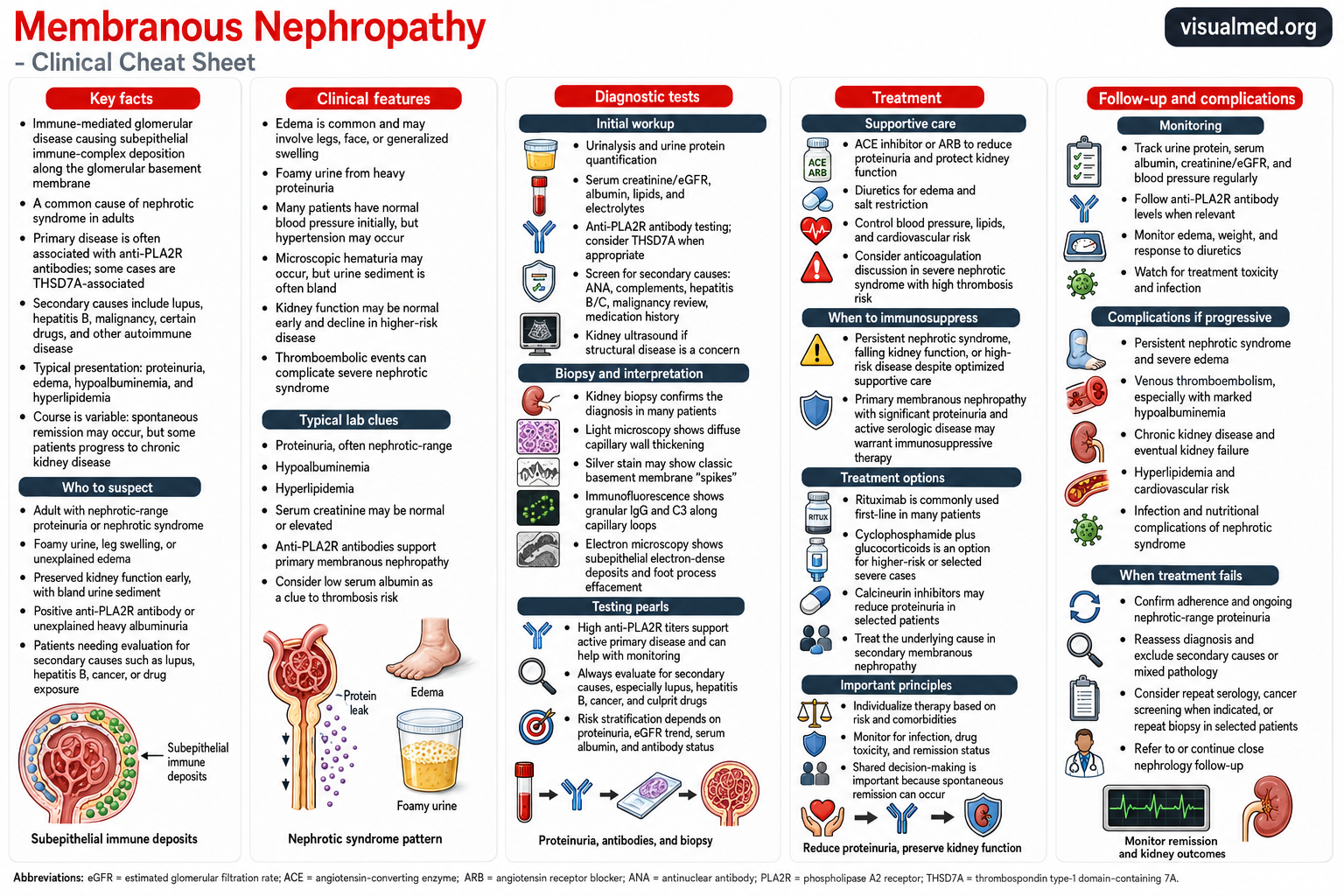
Membranous nephropathy is an immune-mediated disease of the glomeruli—the microscopic filtering units of the kidneys. It develops when antibodies and other immune components accumulate along the outer surface of the glomerular basement membrane, damaging the filtration barrier and allowing large amounts of protein to escape into the urine.
The disease is an important cause of nephrotic syndrome in adults. Its course varies considerably: some patients enter spontaneous remission, while others experience persistent proteinuria, blood clots, declining kidney function, or eventual kidney failure.
What Is Membranous Nephropathy?
Each kidney contains approximately one million nephrons. Within each nephron, a glomerulus filters the blood while normally retaining blood cells and essential proteins.
In membranous nephropathy, immune deposits form beneath the podocytes along the subepithelial side of the glomerular basement membrane. These deposits activate inflammatory pathways and disrupt the podocyte filtration barrier. Albumin and other proteins can then leak from the bloodstream into the urine, producing proteinuria and, in more severe cases, nephrotic syndrome.
Despite the name, the disease does not primarily involve the membranes of the kidney as a whole. “Membranous” refers to the characteristic thickened appearance of the glomerular capillary walls on kidney biopsy.
Primary Versus Secondary Membranous Nephropathy
Membranous nephropathy is classified as either primary or secondary.
Primary membranous nephropathy
Primary membranous nephropathy is an autoimmune disease directed against proteins located on podocytes. The best-known target is the M-type phospholipase A2 receptor, commonly abbreviated PLA2R.
Circulating anti-PLA2R antibodies strongly support the diagnosis of primary membranous nephropathy and can also help assess disease activity and response to treatment. Other target antigens, including THSD7A, are associated with a smaller proportion of cases.
Secondary membranous nephropathy
Secondary disease develops in association with another condition or exposure. Potential causes include:
- Systemic lupus erythematosus
- Hepatitis B or hepatitis C
- Certain cancers
- Nonsteroidal anti-inflammatory drugs
- Other medications or supplements
- Autoimmune and infectious diseases
Every patient diagnosed with membranous nephropathy should undergo a clinically appropriate evaluation for secondary causes, even when anti-PLA2R antibodies are present.
Symptoms and Clinical Presentation
Membranous nephropathy often develops gradually. Some patients are diagnosed after protein is detected during routine urine testing, before obvious symptoms appear.
The most common manifestations are related to urinary protein loss and fluid retention:
- Foamy or frothy urine
- Swelling of the ankles and legs
- Puffiness around the eyes
- Generalized edema in severe cases
- Unexplained weight gain from retained fluid
- Fatigue
- Elevated cholesterol or triglycerides
- Reduced appetite in advanced disease
Blood pressure and kidney function may initially be normal. Microscopic hematuria can occur, although the urinary sediment is often relatively bland compared with more inflammatory forms of glomerulonephritis.
What Is Nephrotic Syndrome?
Membranous nephropathy commonly causes nephrotic syndrome, a clinical pattern characterized by substantial urinary protein loss, low serum albumin, edema, and hyperlipidemia.
Albumin normally helps keep fluid inside the bloodstream. When large quantities of albumin are lost in the urine, fluid moves into the surrounding tissues and produces swelling. The liver also increases lipoprotein production, contributing to elevated cholesterol and triglyceride levels.
Nephrotic syndrome is not simply a problem of swelling. It increases the risk of blood clots, infection, malnutrition, cardiovascular disease, and progressive kidney injury.
Diagnostic Evaluation
The initial evaluation determines how much protein is being lost, how well the kidneys are functioning, and whether an underlying condition is responsible.
Urine testing
Urinalysis can detect protein and blood. Protein loss is then quantified using one of the following:
- Spot urine protein-to-creatinine ratio
- Urine albumin-to-creatinine ratio
- Twenty-four-hour urine protein collection
Protein quantification is important not only for diagnosis but also for risk assessment and treatment monitoring.
Blood testing
Common blood tests include:
- Serum creatinine and estimated glomerular filtration rate
- Serum albumin
- Electrolytes
- Cholesterol and triglycerides
- Anti-PLA2R antibodies
- Antinuclear antibodies and complement levels when lupus is possible
- Hepatitis B and C testing
- Additional testing guided by medications, symptoms, age, and cancer-screening history
A falling albumin level and persistent heavy proteinuria indicate more severe nephrotic syndrome and may signal a higher thrombotic risk.
The Role of Anti-PLA2R Antibodies
Anti-PLA2R testing has transformed the diagnosis and monitoring of membranous nephropathy.
In a patient with nephrotic syndrome, normal or reasonably preserved kidney function, and a positive anti-PLA2R antibody result, KDIGO states that kidney biopsy is not always required to establish the diagnosis. Biopsy may nevertheless remain valuable when the clinical course is unusual, kidney function is falling rapidly, another systemic disease is suspected, or the response to treatment is unexpected.
A negative blood test does not completely exclude PLA2R-associated disease. Antibodies may be absent early, may have already fallen by the time of testing, or may be detectable within kidney tissue even when the serum test is negative.
Antibody levels are also useful during treatment. An immunologic response, reflected by falling or disappearing antibodies, often occurs months before the full improvement in proteinuria becomes apparent.
Kidney Biopsy Findings
When performed, a kidney biopsy can confirm membranous nephropathy, assess chronic damage, identify another glomerular disease, and sometimes help distinguish primary from secondary disease.
Characteristic findings include:
- Diffuse thickening of glomerular capillary walls on light microscopy
- “Spike” formation along the basement membrane on silver staining
- Granular IgG and C3 deposition along the capillary loops on immunofluorescence
- Subepithelial electron-dense deposits on electron microscopy
- Podocyte foot-process effacement
Biopsy tissue may also be stained for PLA2R and other antigens. Positive glomerular PLA2R staining can identify PLA2R-associated membranous nephropathy even when circulating antibodies are not detected.
Assessing the Risk of Disease Progression
Treatment is not based on proteinuria alone. Clinicians consider several findings together:
- Amount and duration of proteinuria
- Serum albumin
- Changes in creatinine and eGFR
- Anti-PLA2R antibody levels
- Complications of nephrotic syndrome
- Biopsy evidence of chronic kidney damage
- Age and accompanying medical conditions
Patients with stable kidney function and improving proteinuria may be managed initially with supportive therapy and close observation. Immunosuppression is generally reserved for patients with moderate, high, or very high risk of progression or serious nephrotic complications.
Supportive Treatment
Every patient should receive treatment directed at the consequences of proteinuria and nephrotic syndrome.
ACE inhibitors and ARBs
An ACE inhibitor or angiotensin receptor blocker can lower intraglomerular pressure, reduce urinary protein loss, control blood pressure, and help protect kidney function.
Diuretics and sodium restriction
Diuretics help remove excess fluid and control edema. Reducing dietary sodium can improve the response to diuretics and limit recurrent fluid retention. Severe edema may require careful combination diuretic therapy under medical supervision.
Cardiovascular risk management
Nephrotic syndrome frequently causes marked hyperlipidemia. Blood pressure, lipid levels, smoking, diabetes, exercise, and other cardiovascular risk factors should be addressed as part of long-term kidney care.
Blood-Clot Risk and Anticoagulation
Membranous nephropathy carries a particularly important risk of venous and arterial thromboembolic events. Possible complications include deep-vein thrombosis, pulmonary embolism, and renal-vein thrombosis.
The risk rises as serum albumin falls and nephrotic syndrome becomes more severe. KDIGO advises considering preventive anticoagulation in selected patients with low serum albumin after weighing the estimated clotting risk against the individual risk of serious bleeding. This decision should not be based on albumin alone and requires individualized clinical assessment.
When Is Immunosuppressive Treatment Needed?
Immunosuppressive treatment may be appropriate when a patient has:
- Persistent nephrotic syndrome
- Substantial or rising anti-PLA2R antibody levels
- Declining kidney function attributable to active disease
- Severe proteinuria despite optimized supportive care
- Serious complications of nephrotic syndrome
- A high predicted risk of progressive kidney disease
Because spontaneous remission can occur, patients at low risk are generally not exposed immediately to potentially toxic immunosuppressive drugs. KDIGO recommends selecting therapy according to the patient’s overall risk category rather than using one regimen for every patient.
Rituximab
Rituximab is a monoclonal antibody that targets CD20-positive B lymphocytes, reducing the production of pathogenic antibodies. It is now an important treatment option for primary membranous nephropathy in patients who require immunosuppression.
In the randomized MENTOR trial, rituximab was noninferior to cyclosporine for inducing complete or partial proteinuria remission at 12 months and was superior for maintaining remission through 24 months. The longer-term advantage was largely related to fewer relapses after treatment compared with cyclosporine.
Response is not immediate. Anti-PLA2R antibodies may fall first, followed later by improvement in serum albumin and proteinuria.
Cyclophosphamide and Glucocorticoids
Alternating or combined cyclophosphamide and glucocorticoid regimens remain an important option, particularly for high-risk or very-high-risk disease.
This approach can produce durable remission but has significant potential toxicity, including infection, bone-marrow suppression, infertility, bladder injury, and increased malignancy risk. Treatment therefore requires careful patient selection, dose monitoring, and counseling. KDIGO particularly prioritizes cyclophosphamide-based treatment for patients at very high risk of kidney-function loss.
Calcineurin Inhibitors
Tacrolimus or cyclosporine can reduce proteinuria relatively quickly. However, relapse may occur when treatment is withdrawn, and prolonged therapy can cause hypertension and kidney toxicity.
Calcineurin inhibitors may be used in selected patients, sometimes in combination with rituximab or glucocorticoids depending on the risk category and treatment strategy.
Treating Secondary Membranous Nephropathy
When membranous nephropathy is secondary to another disease or exposure, treatment should focus on the underlying cause whenever possible.
Examples include:
- Treating hepatitis B or another infection
- Managing systemic lupus erythematosus
- Discontinuing an implicated medication
- Evaluating and treating an associated malignancy
- Addressing another autoimmune disorder
The immunosuppressive strategy used for primary membranous nephropathy may not be appropriate until the secondary cause has been identified and considered.
Monitoring and Follow-Up
Membranous nephropathy requires ongoing follow-up even when symptoms improve. Monitoring typically includes:
- Urine protein excretion
- Serum albumin
- Creatinine and eGFR
- Blood pressure
- Body weight and edema
- Anti-PLA2R antibody levels when applicable
- Medication toxicity
- Signs of infection or thromboembolism
Clinical improvement may lag behind immunologic improvement. Persistent proteinuria does not always mean that active autoimmune disease remains, particularly when anti-PLA2R antibodies have disappeared and serum albumin has normalized. In this situation, clinicians may need to consider residual structural damage or secondary focal segmental glomerulosclerosis rather than automatically escalating immunosuppression.
Potential Complications
Progressive or severe membranous nephropathy may lead to:
- Persistent nephrotic syndrome
- Severe or recurrent edema
- Deep-vein thrombosis or pulmonary embolism
- Renal-vein thrombosis
- Infection
- Malnutrition
- Hyperlipidemia and cardiovascular disease
- Acute kidney injury
- Chronic kidney disease
- Kidney failure requiring dialysis or transplantation
Some patients respond well to supportive care or immunosuppression and maintain kidney function for many years. Others experience relapses or gradual progression, making regular nephrology follow-up essential.
Key Takeaway
Membranous nephropathy is an immune-mediated glomerular disease that commonly presents with heavy proteinuria, low serum albumin, edema, and hyperlipidemia.
Anti-PLA2R antibody testing can support the diagnosis, help determine disease activity, and monitor response to therapy. Kidney biopsy remains important when antibody testing is negative, the presentation is unusual, kidney function is declining, or another diagnosis is possible.
All patients require supportive kidney-protective care. Immunosuppressive treatment—such as rituximab, cyclophosphamide with glucocorticoids, or a calcineurin inhibitor—is reserved for patients whose risk of progressive disease or nephrotic complications outweighs the potential toxicity of therapy.
This article is intended for medical education and does not replace individualized assessment or treatment by a nephrologist or other qualified healthcare professional.