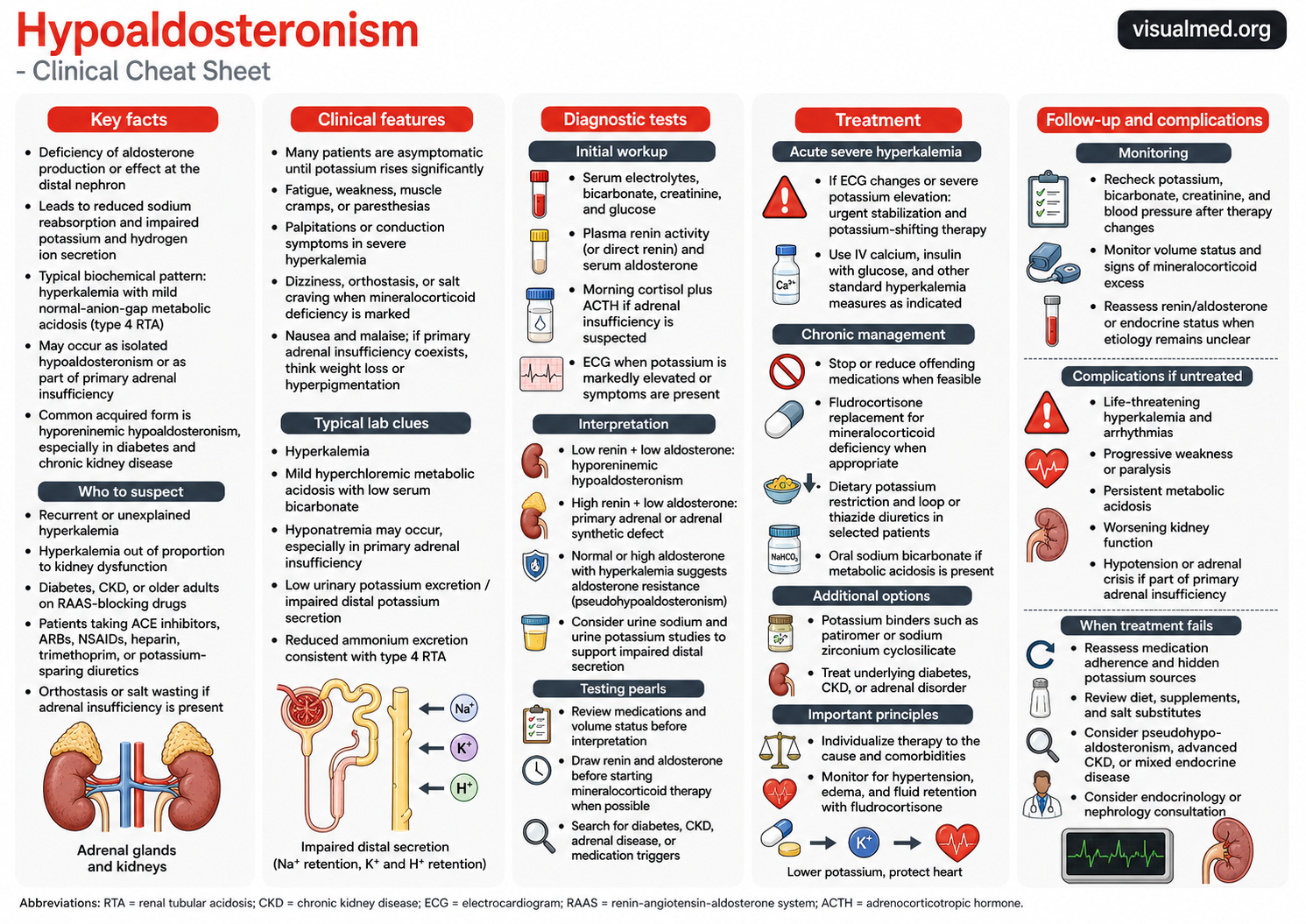
What is hypoaldosteronism?
Hypoaldosteronism is a condition in which aldosterone production or aldosterone effect is reduced. Aldosterone normally acts at the distal nephron to promote sodium reabsorption and potassium and hydrogen ion secretion. When aldosterone is deficient or ineffective, patients can develop hyperkalemia and a mild normal-anion-gap metabolic acidosis, often described as type 4 renal tubular acidosis. (Merck Manuals)
The key clinical pattern is:
Low aldosterone effect → impaired distal potassium secretion → hyperkalemia ± metabolic acidosis.
This is especially important because the patient may look well, have only mild kidney dysfunction, and still have potassium levels that are disproportionately high.
Why aldosterone matters
Aldosterone is a mineralocorticoid hormone produced by the adrenal zona glomerulosa. Its job is to help the kidney retain sodium and excrete potassium. When aldosterone signaling is inadequate, potassium excretion falls. Hyperkalemia also reduces renal ammonium generation, contributing to impaired acid excretion and type 4 RTA. (NCBI)
That is why hypoaldosteronism often presents with the combination of:
Hyperkalemia
Low serum bicarbonate
Hyperchloremic normal-anion-gap metabolic acidosis
Relatively mild renal dysfunction
Major causes of hypoaldosteronism
Hypoaldosteronism can be divided into three practical categories.
1. Low renin and low aldosterone
This is classically seen in hyporeninemic hypoaldosteronism, the most common acquired form. It is particularly associated with diabetes mellitus, chronic kidney disease, and older age. Endotext notes that hyporeninemic hypoaldosteronism should be considered in patients with unexplained hyperkalemia after evaluating renal function and excluding drugs that impair potassium excretion. (NCBI)
Common settings include:
Diabetic kidney disease
Chronic kidney disease
Older adults
Autonomic dysfunction
Use of RAAS-blocking drugs
2. High renin and low aldosterone
This pattern suggests the kidney is trying to stimulate aldosterone production, but the adrenal gland is not responding appropriately. Causes include primary adrenal insufficiency, adrenal destruction, adrenal enzyme defects, or aldosterone synthase defects.
In these patients, look for additional features of adrenal insufficiency, such as hypotension, weight loss, salt craving, nausea, hyperpigmentation, or hyponatremia.
3. Normal or high aldosterone with impaired effect
This suggests aldosterone resistance, sometimes called pseudohypoaldosteronism. In this situation, aldosterone may be present, but the distal nephron does not respond appropriately.
Clinical features
Many patients with hypoaldosteronism are asymptomatic until potassium becomes significantly elevated. Symptoms, when present, are usually driven by hyperkalemia, salt wasting, or adrenal insufficiency.
Possible symptoms include:
Fatigue
Weakness
Muscle cramps
Paresthesias
Palpitations
Dizziness or orthostasis
Salt craving
Nausea or malaise
Severe hyperkalemia can cause cardiac conduction abnormalities and life-threatening arrhythmias, so symptoms such as palpitations, syncope, profound weakness, or ECG changes require urgent evaluation.
When to suspect hypoaldosteronism
Think about hypoaldosteronism when the potassium is repeatedly high and the explanation is not obvious.
Clinical clues include:
Recurrent or unexplained hyperkalemia
Hyperkalemia out of proportion to kidney dysfunction
Mild normal-anion-gap metabolic acidosis
Diabetes or chronic kidney disease
Use of ACE inhibitors, ARBs, NSAIDs, heparin, trimethoprim, calcineurin inhibitors, or potassium-sparing diuretics
Low urinary potassium excretion despite hyperkalemia
Features of adrenal insufficiency
Medication review is essential because many common drugs can reduce aldosterone production, block the RAAS pathway, or impair renal potassium excretion.
Diagnostic workup
The first step is to confirm the biochemical pattern and assess severity.
Initial tests usually include:
Serum potassium
Sodium, chloride, and bicarbonate
Creatinine and estimated GFR
Glucose
Serum magnesium if clinically relevant
ECG if potassium is markedly elevated or symptoms are present
The key hormonal tests are:
Plasma renin activity or direct renin
Serum aldosterone
These should ideally be interpreted before starting mineralocorticoid therapy, because treatment can alter the results.
A practical interpretation:
Low renin + low aldosterone
Suggests hyporeninemic hypoaldosteronism.
High renin + low aldosterone
Suggests primary adrenal aldosterone deficiency or adrenal synthetic impairment.
Normal/high aldosterone + hyperkalemia
Suggests aldosterone resistance or impaired distal nephron response.
If adrenal insufficiency is possible, add:
Morning cortisol
ACTH
Possible cosyntropin stimulation testing depending on context
Urine studies can help support impaired distal potassium secretion, especially when the diagnosis is unclear.
Treatment approach
Treatment depends on potassium severity, ECG findings, symptoms, kidney function, volume status, blood pressure, and the underlying cause.
Acute severe hyperkalemia
If the patient has ECG changes, severe hyperkalemia, or concerning symptoms, management should follow standard urgent hyperkalemia treatment protocols. This may include IV calcium for membrane stabilization, insulin with glucose to shift potassium intracellularly, beta-agonists, bicarbonate in selected acidotic patients, potassium binders, diuretics, or dialysis when indicated.
Chronic management
For stable patients, the goal is to reduce recurrent hyperkalemia and correct the underlying disorder.
Key steps include:
Review and stop offending medications when feasible
Reduce dietary potassium intake when appropriate
Use loop or thiazide diuretics in selected patients
Treat metabolic acidosis with oral sodium bicarbonate when present
Use potassium binders such as patiromer or sodium zirconium cyclosilicate when needed
Treat underlying diabetes, CKD, or adrenal disease
Fludrocortisone can be useful when true mineralocorticoid deficiency is present, but it requires caution because it can cause sodium retention, hypertension, edema, fluid overload, and worsening heart failure risk. (NCBI)
Follow-up and monitoring
After treatment changes, follow-up should focus on potassium control, acid-base status, kidney function, and blood pressure.
Monitor:
Serum potassium
Bicarbonate
Creatinine/eGFR
Blood pressure
Volume status
Edema or signs of mineralocorticoid excess
Medication adherence
Dietary potassium intake
Use of salt substitutes or supplements
If hyperkalemia persists despite treatment, revisit the diagnosis. Consider hidden potassium sources, advanced CKD, aldosterone resistance, medication interactions, or mixed endocrine disease.
Complications if untreated
Untreated hypoaldosteronism can lead to:
Persistent hyperkalemia
Cardiac conduction abnormalities
Life-threatening arrhythmias
Muscle weakness or paralysis
Chronic metabolic acidosis
Worsening kidney function
Hypotension or adrenal crisis if part of primary adrenal insufficiency
The most dangerous complication is severe hyperkalemia, particularly when it affects cardiac conduction.
Clinical takeaway
Hypoaldosteronism is a high-yield diagnosis to consider in patients with recurrent hyperkalemia, especially when the degree of hyperkalemia seems worse than expected for the level of kidney dysfunction. The classic clue is hyperkalemia with mild normal-anion-gap metabolic acidosis, often in a patient with diabetes, CKD, or exposure to RAAS-blocking medications.
The practical approach is:
Recognize the pattern.
Review medications.
Check renin and aldosterone.
Treat hyperkalemia based on severity.
Individualize long-term therapy to the cause, blood pressure, volume status, and kidney function.
References
- Endotext. Aldosterone Deficiency and Resistance. NCBI Bookshelf. (NCBI)
- Merck Manual Professional Edition. Renal Tubular Acidosis. (Merck Manuals)
- StatPearls. Renal Tubular Acidosis. NCBI Bookshelf. (NCBI)
- Sousa AGP et al. Hyporeninemic hypoaldosteronism and diabetes mellitus. PMC. (PMC)
- StatPearls. Hypoaldosteronism. NCBI Bookshelf. (NCBI)