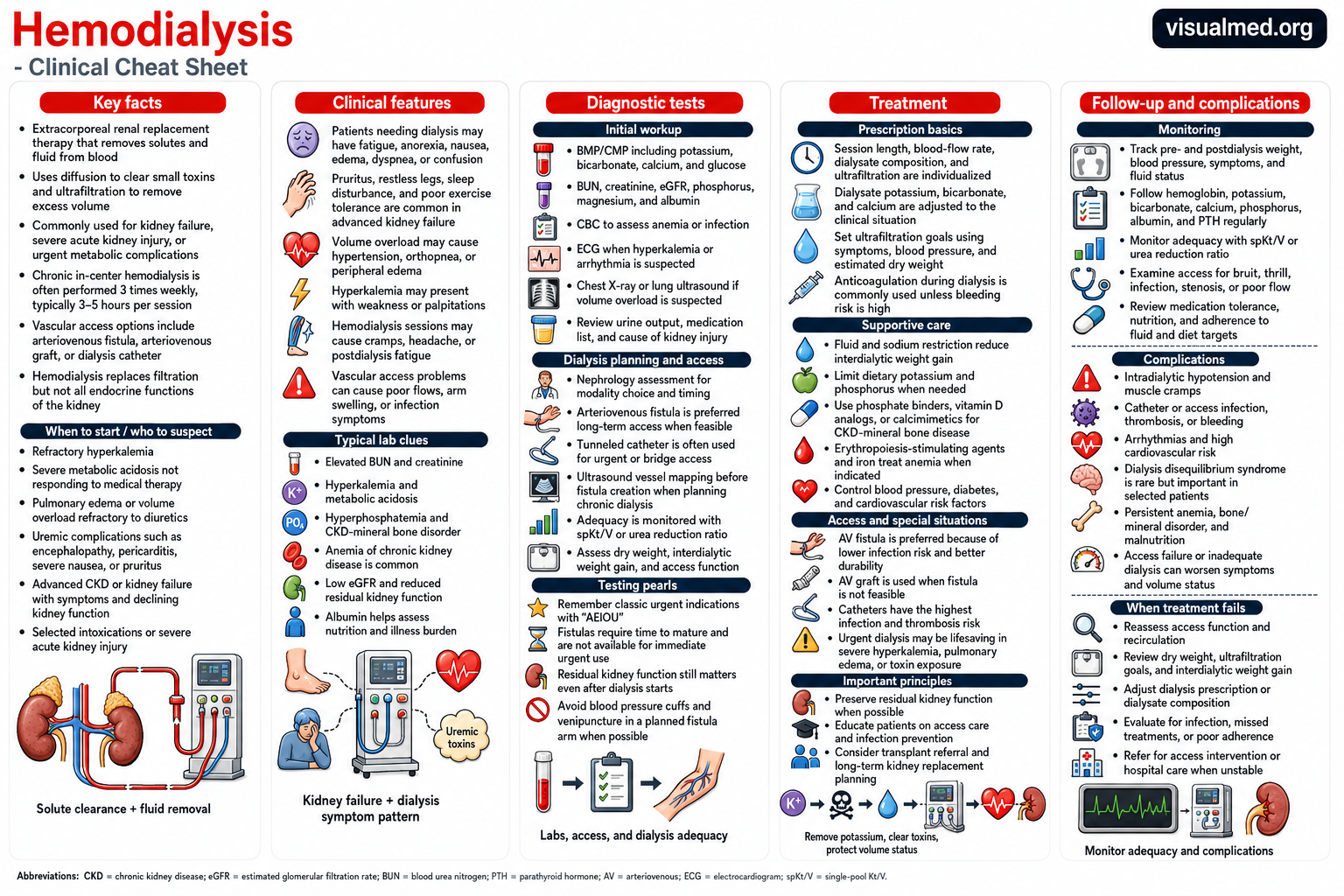
Hemodialysis is an extracorporeal kidney replacement therapy that removes accumulated solutes and excess extracellular fluid while correcting selected electrolyte and acid-base abnormalities. Blood is circulated through a dialyzer containing a semipermeable membrane, across which solutes are cleared primarily by diffusion and fluid is removed by ultrafiltration.
Although conventional maintenance hemodialysis is often delivered three times weekly, the schedule, session duration, dialysate composition, blood-flow rate, and ultrafiltration prescription should be individualized. Dialysis replaces part of the kidney’s excretory function, but it does not fully reproduce continuous volume regulation, endocrine activity, or native tubular physiology.
When Should Hemodialysis Be Initiated?
There is no universally accepted eGFR threshold at which maintenance dialysis should automatically begin. KDIGO recommends basing initiation on the overall clinical picture rather than starting preemptively because the eGFR has crossed a particular numerical value. Relevant factors include symptom burden, biochemical abnormalities, volume status, nutritional trajectory, functional status, comorbidities, and patient goals.
Dialysis is generally considered when one or more of the following are present:
- Neurologic manifestations of uremia, including encephalopathy
- Uremic pericarditis
- Medically refractory hyperkalemia or other electrolyte disturbances
- Persistent metabolic acidosis despite appropriate medical management
- Pulmonary edema or extracellular volume overload that cannot be controlled medically
- Inability to control blood pressure because of volume excess
- Progressive anorexia, weight loss, or protein-energy wasting
- Severe, refractory pruritus, nausea, bleeding, or other symptoms attributable to kidney failure
KDIGO specifically identifies kidney-failure symptoms, resistant electrolyte or acid-base abnormalities, inability to control volume or blood pressure, and progressive nutritional deterioration despite intervention as major reasons to initiate maintenance dialysis.
The traditional AEIOU mnemonic—acidosis, electrolyte abnormalities, intoxications, overload, and uremia—remains useful for recalling urgent indications, but it should not replace clinical judgment.
In acute kidney injury, kidney replacement therapy should be initiated emergently when life-threatening fluid, electrolyte, or acid-base abnormalities are present. Trends, reversibility, hemodynamics, urine output, catabolic state, and the broader clinical context are more informative than isolated BUN or creatinine values.
Planning Before Kidney Failure
Preparation for kidney replacement therapy should begin well before dialysis is required. The KDIGO 2024 CKD guideline suggests that a two-year kidney-failure risk above 40% can help determine when to begin modality education, transplantation referral, and vascular-access planning, in addition to eGFR, the rate of progression, and other clinical considerations.
Predialysis counseling should address:
- In-center versus home hemodialysis
- Peritoneal dialysis
- Preemptive kidney transplantation
- Expected treatment burden and prognosis
- Vascular-access options
- Conservative kidney management when appropriate
- The patient’s functional, occupational, and quality-of-life priorities
The objective is not merely to create an access. It is to establish a coherent kidney-failure plan that reflects expected survival, comorbidities, vascular anatomy, transplant candidacy, home support, and patient preferences.
Initial Clinical and Laboratory Assessment
Before initiating hemodialysis, clinicians should establish the indication, urgency, potentially reversible contributors, and the safest modality.
A typical evaluation includes:
- Serum potassium, bicarbonate, sodium, calcium, magnesium, and glucose
- BUN, creatinine, and serial kidney-function trends
- Phosphorus and albumin
- Complete blood count and iron indices
- Urinalysis, urine output, and residual kidney function
- ECG when hyperkalemia, ischemia, or arrhythmia is suspected
- Chest imaging or lung ultrasonography when pulmonary congestion is uncertain
- Medication review, including renally cleared agents and nephrotoxins
- Assessment of volume status, nutrition, cognition, frailty, and functional trajectory
In AKI, the cause and expected potential for recovery must remain under active review after dialysis begins. Kidney replacement therapy should be discontinued when native function has recovered sufficiently to meet clinical needs or when treatment is no longer consistent with the goals of care.
Vascular-Access Selection
The three principal hemodialysis access types are the arteriovenous fistula, arteriovenous graft, and central venous catheter.
Arteriovenous fistula
An AV fistula generally offers good long-term durability and lower infection risk when it matures successfully. It requires suitable vascular anatomy and adequate time for maturation.
Arteriovenous graft
An AV graft can often be cannulated sooner and may be appropriate when native vessels are unlikely to support a functional fistula. It carries higher thrombosis and infection risks than a mature fistula but usually less bloodstream-infection risk than a catheter.
Central venous catheter
A dialysis catheter provides immediate access and is frequently required during an urgent or unplanned start. However, catheters have substantial risks of bloodstream infection, thrombosis, poor blood flow, central venous stenosis, and inadequate dialysis delivery. CDC guidance emphasizes reducing catheter exposure when a suitable lower-risk access is available and applying standardized infection-prevention procedures whenever catheters are used.
Modern KDOQI guidance has moved away from an indiscriminate “fistula first” strategy toward the ESKD Life-Plan. Access selection should account for the patient’s anticipated modality, vascular anatomy, life expectancy, comorbidities, prior access history, transplant prospects, and individual treatment goals.
Hemodialysis Prescription Fundamentals
A conventional prescription includes the treatment frequency and duration, dialyzer, blood-flow rate, dialysate-flow rate, dialysate composition, anticoagulation strategy, temperature, and ultrafiltration target.
Treatment time and frequency
For patients with little residual kidney function receiving thrice-weekly dialysis, KDOQI recommends at least three hours per session. Longer or additional sessions should be considered when patients have large interdialytic weight gains, high ultrafiltration requirements, uncontrolled blood pressure, difficulty reaching target weight, persistent hyperkalemia, acidosis, or hyperphosphatemia.
Dialysate composition
Dialysate potassium should be selected according to the predialysis potassium level, arrhythmia risk, dietary pattern, residual kidney function, and likelihood of postdialysis rebound. Abrupt serum-to-dialysate potassium gradients may contribute to electrophysiologic instability, whereas an excessively high dialysate potassium may provide inadequate removal.
Dialysate bicarbonate should correct chronic acid retention while avoiding excessive postdialysis alkalemia. Dialysate calcium must be individualized according to hemodynamics, mineral-bone status, arrhythmia risk, and concurrent medications.
Anticoagulation
Unfractionated heparin is commonly used during intermittent hemodialysis. The regimen should be modified or withheld in patients with active bleeding, severe thrombocytopenia, recent high-risk surgery, heparin-induced thrombocytopenia, or other contraindications. In AKI, KDIGO recommends balancing anticoagulation benefits against bleeding risk and using an alternative strategy when heparin is contraindicated.
Dialysis Adequacy
Urea clearance remains the conventional quantitative measure of delivered hemodialysis dose. For patients treated three times weekly, KDOQI recommends a target single-pool Kt/V of 1.4 per session, with a minimum delivered spKt/V of 1.2. Patients with significant residual native kidney function may receive a modified prescription provided that residual clearance is measured periodically.
Adequacy should not be reduced to Kt/V alone. A patient may meet a urea-clearance target while remaining inadequately treated because of:
- Persistent volume overload
- Poor blood-pressure control
- Ongoing hyperkalemia or acidosis
- Malnutrition or progressive weight loss
- Uncontrolled uremic symptoms
- Recurrent access dysfunction
- Severe postdialysis fatigue or hypotension
- Inadequate middle-molecule or phosphorus control
Conversely, an unexpectedly low Kt/V should prompt assessment for shortened treatments, low blood-flow rates, access recirculation, needle-position problems, dialyzer clotting, inadequate dialyzer size, inaccurate blood sampling, or access stenosis.
Volume and Blood-Pressure Management
Determining and maintaining an appropriate target weight is central to hemodialysis care. The target is dynamic and may change with nutrition, intercurrent illness, cardiac function, residual kidney function, hospitalization, and changes in body composition.
Ultrafiltration should balance the need to achieve euvolemia against the risks of intradialytic hypotension, myocardial and cerebral hypoperfusion, cramping, ischemic injury, and accelerated loss of residual kidney function. KDIGO emphasizes that volume and blood-pressure management require individualized consideration of comorbidities, hemodynamic patterns, symptoms, lifestyle, and patient priorities.
Recurrent intradialytic hypotension should trigger review of:
- Target weight
- Interdialytic weight gain
- Ultrafiltration rate and treatment duration
- Pre-dialysis antihypertensive timing
- Dialysate temperature and sodium
- Cardiac function and autonomic disease
- Active infection, bleeding, or poor nutrition
- Food intake during treatment
Increasing treatment duration or frequency is often preferable to attempting aggressive fluid removal over an insufficient treatment time.
Supportive Management Between Treatments
Hemodialysis should be integrated with treatment of the broader consequences of kidney failure.
Fluid, sodium, potassium, and phosphorus
Dietary sodium and fluid intake should be aligned with urine output, interdialytic weight gain, blood pressure, and the prescribed dialysis schedule. Potassium restriction should be individualized rather than applied uniformly, with attention to medications, constipation, glycemic control, tissue breakdown, and dialysate potassium.
Phosphate-lowering treatment should be based on persistent or progressive hyperphosphatemia. The selection of a phosphate binder should consider calcium levels, pill burden, vascular calcification, PTH status, cost, and treatment adherence. Management of secondary hyperparathyroidism may include vitamin D receptor activators, calcimimetics, or combined therapy in appropriate patients.
Anemia
The evaluation of anemia in a patient receiving hemodialysis should address iron deficiency, inflammation, occult blood loss, inadequate dialysis, hyperparathyroidism, nutritional deficiencies, and bone-marrow disease before escalating an erythropoiesis-stimulating agent.
The KDIGO 2026 anemia guideline considers a hemoglobin of approximately 9–10 g/dL a reasonable range at which to consider ESA initiation in maintenance-dialysis patients, with individualization according to symptoms, transfusion avoidance, cardiovascular risk, prior stroke, and vascular-access thrombosis. Higher hemoglobin targets should be avoided because they increase cardiovascular and vascular-access risk.
Routine Monitoring
Clinical review should integrate dialysis-unit data with longitudinal symptoms and examination findings.
Important parameters include:
- Pre- and postdialysis weight and blood pressure
- Interdialytic weight gain
- Orthostatic and intradialytic symptoms
- Potassium, bicarbonate, calcium, phosphorus, and albumin
- Hemoglobin and iron indices
- PTH and alkaline phosphatase
- Delivered spKt/V or urea reduction ratio
- Residual urine output when present
- Nutritional and functional status
- Medication reconciliation
- Access examination and treatment pressures
An AV fistula or graft should be assessed for thrill, bruit, pulse characteristics, arm edema, prolonged bleeding, difficult cannulation, and changes in arterial or venous pressures. Catheters should be evaluated for exit-site infection, tunnel tenderness, poor flow, and systemic infection.
Common Hemodialysis Complications
Intradialytic hypotension
Potential contributors include excessive ultrafiltration, incorrect target weight, impaired cardiac reserve, autonomic dysfunction, vasodilator medications, eating during treatment, and sepsis.
Muscle cramps
Cramps commonly accompany rapid volume removal or hypotension. Management should focus on reassessing ultrafiltration and volume targets rather than repeatedly treating symptoms without correcting the prescription.
Arrhythmias
Rapid changes in potassium, calcium, pH, and volume can contribute to atrial and ventricular arrhythmias, particularly in patients with structural heart disease.
Access infection and thrombosis
Access infection must be assessed promptly, with blood cultures, antimicrobial therapy, and source-control decisions guided by access type and clinical severity. CDC’s core interventions include surveillance, hand-hygiene audits, standardized catheter-care observations, staff competency assessment, and patient education.
Dialysis disequilibrium syndrome
Dialysis disequilibrium syndrome is uncommon but should be considered in severely uremic patients who develop headache, nausea, agitation, confusion, seizures, or cerebral edema during or shortly after initial treatment. Prevention relies on a cautious initial prescription with slower solute removal in high-risk patients.
When Hemodialysis Appears to Be Failing
Persistent symptoms or abnormal laboratory values should prompt a systematic reassessment rather than automatic escalation of dialysis time.
Evaluate:
- Whether the prescribed treatments are being completed.
- Vascular-access function and possible recirculation.
- Delivered blood-flow and dialysate-flow rates.
- Dialyzer performance and clotting.
- Target weight and ultrafiltration tolerance.
- Dialysate potassium, calcium, sodium, and bicarbonate.
- Dietary intake and medication adherence.
- Infection, inflammation, cardiac disease, or another nondialysis cause of symptoms.
- Whether a different schedule, home modality, peritoneal dialysis, or transplantation would better meet the patient’s goals.
Key Takeaway
Hemodialysis is not simply initiated at a particular creatinine or eGFR and is not adequately managed by achieving a Kt/V target alone.
High-quality hemodialysis care requires:
- Symptom- and context-based initiation
- Early modality and access planning
- A patient-specific vascular-access strategy
- Individualized solute and fluid prescriptions
- Active preservation of residual kidney function
- Continuous assessment of volume, cardiovascular risk, nutrition, anemia, mineral-bone disease, and access integrity
- Repeated alignment of treatment with the patient’s broader kidney-failure life plan
This article is intended for clinician education and should be applied alongside nephrology consultation, local protocols, and individualized clinical judgment.