What is Cushing syndrome?
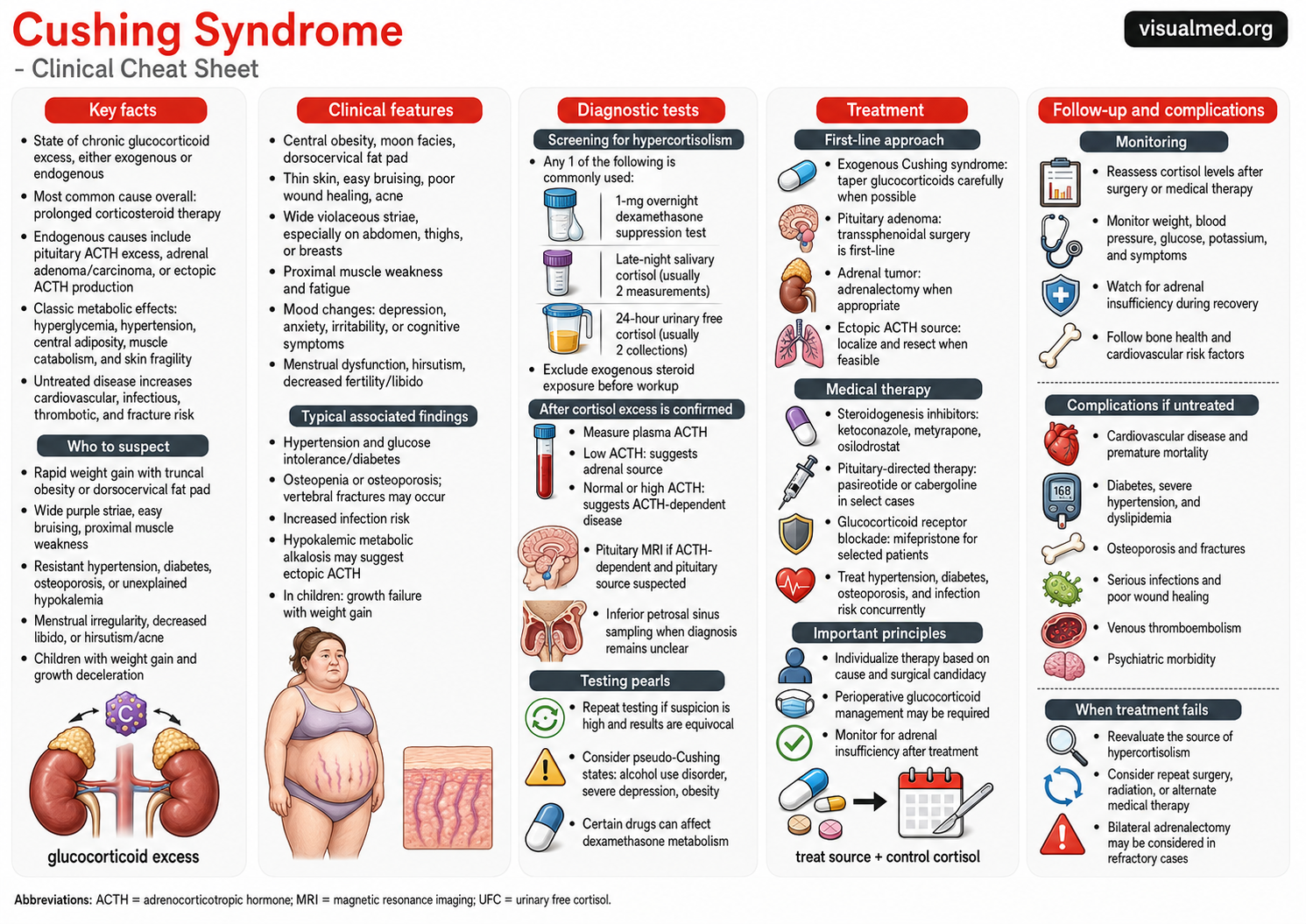
Cushing syndrome is the clinical state caused by chronic exposure to excess glucocorticoids, most commonly cortisol. It can be caused by exogenous steroid use or by endogenous overproduction of cortisol from the pituitary, adrenal glands, or ectopic ACTH-secreting tumors. The most common cause overall is prolonged glucocorticoid therapy. (NIDDK)
The key concept is simple:
Too much cortisol → metabolic dysfunction, muscle and skin catabolism, immune suppression, hypertension, diabetes, osteoporosis, and cardiovascular risk.
Cushing syndrome is important because the diagnosis is often delayed. Many findings, such as weight gain, hypertension, diabetes, mood changes, and fatigue, are common in the general population. The diagnosis becomes more likely when these features are progressive, clustered, and accompanied by discriminatory signs such as wide purple striae, proximal muscle weakness, easy bruising, facial plethora, or unexplained osteoporosis.
Cushing syndrome vs Cushing disease
These terms are related but not identical.
Cushing syndrome refers to any cause of chronic glucocorticoid excess.
Cushing disease specifically refers to an ACTH-secreting pituitary adenoma causing cortisol excess.
So, all Cushing disease is Cushing syndrome, but not all Cushing syndrome is Cushing disease.
Major causes
Cushing syndrome can be divided into exogenous and endogenous causes.
Exogenous Cushing syndrome
This is the most common cause overall. It results from chronic use of glucocorticoids such as prednisone, methylprednisolone, dexamethasone, hydrocortisone, or high-dose inhaled, topical, intra-articular, or epidural steroids.
Before ordering a large endocrine workup, always ask carefully about steroid exposure.
Endogenous Cushing syndrome
Endogenous causes include:
Pituitary ACTH excess
This is Cushing disease.
Adrenal cortisol production
This includes adrenal adenoma, adrenal carcinoma, or adrenal hyperplasia.
Ectopic ACTH production
This can occur with tumors such as small cell lung cancer, bronchial carcinoid tumors, pancreatic neuroendocrine tumors, and others.
Clinical features
Cortisol excess affects nearly every organ system.
Common clinical features include:
Central weight gain with truncal obesity
Moon facies and facial plethora
Dorsocervical fat pad
Wide violaceous striae, especially on the abdomen, thighs, or breasts
Thin skin, easy bruising, and poor wound healing
Proximal muscle weakness, especially difficulty rising from a chair or climbing stairs
Hypertension
Glucose intolerance or diabetes
Mood changes, depression, anxiety, irritability, or cognitive symptoms
Menstrual irregularity, infertility, low libido, acne, or hirsutism
Osteopenia, osteoporosis, or vertebral compression fractures
Increased infection risk
In children, one of the classic clues is weight gain with growth deceleration.
When to suspect Cushing syndrome
The Endocrine Society recommends testing patients with multiple and progressive features compatible with Cushing syndrome, especially those with more discriminatory features, and patients with adrenal incidentalomas when clinically appropriate. (OUP Academic)
Think about Cushing syndrome when you see:
Rapid central weight gain
Wide purple striae
Easy bruising without clear explanation
Proximal muscle weakness
Resistant hypertension
Diabetes that is difficult to control
Unexplained osteoporosis or fragility fracture
Hypokalemia, especially if severe or associated with suspected ectopic ACTH
Menstrual dysfunction, hirsutism, or acne
Growth failure with weight gain in children
The key is not one isolated feature. The clue is the pattern.
Initial diagnostic testing
Before testing, first exclude exogenous glucocorticoid exposure. This includes oral, inhaled, topical, injected, and over-the-counter steroid-containing products.
The Endocrine Society recommends using one of several high-accuracy screening tests for suspected Cushing syndrome: 24-hour urinary free cortisol, late-night salivary cortisol, 1-mg overnight dexamethasone suppression test, or 2-mg 48-hour dexamethasone suppression test. (Endocrine)
Common first-line screening options:
1-mg overnight dexamethasone suppression test
The patient takes dexamethasone at night, and serum cortisol is measured the next morning. Failure to suppress suggests hypercortisolism.
Late-night salivary cortisol
Cortisol should normally be low late at night. Elevated late-night salivary cortisol suggests loss of normal diurnal rhythm. This is often collected twice.
24-hour urinary free cortisol
This measures free cortisol excretion over 24 hours. It is often collected twice because cortisol secretion can vary.
Random serum cortisol is generally not a good screening test because cortisol normally fluctuates throughout the day.
After hypercortisolism is confirmed
Once cortisol excess is confirmed, the next step is to determine the source.
The practical branch point is plasma ACTH.
Low ACTH suggests an adrenal source, such as adrenal adenoma, carcinoma, or hyperplasia.
Normal or high ACTH suggests ACTH-dependent disease, usually pituitary Cushing disease or ectopic ACTH production.
Further testing may include pituitary MRI, adrenal CT or MRI, chest/abdomen imaging for ectopic ACTH sources, and inferior petrosal sinus sampling when the source remains unclear.
Pseudo-Cushing states and testing pitfalls
Several conditions can mimic biochemical or clinical Cushing syndrome. These are sometimes called pseudo-Cushing states.
Examples include:
Alcohol use disorder
Severe depression or psychiatric illness
Obesity
Poorly controlled diabetes
Severe physiologic stress
Pregnancy
Untreated obstructive sleep apnea
Testing can also be affected by medications. Drugs that alter dexamethasone metabolism can produce misleading dexamethasone suppression test results. Cyclic Cushing syndrome can also cause fluctuating results, so repeat testing may be necessary when clinical suspicion remains high.
Treatment
Treatment depends on the cause.
For endogenous Cushing syndrome, the Endocrine Society recommends removal of the causative tumor as first-line treatment unless surgery is not possible or unlikely to correct the cortisol excess. (Endocrine)
Exogenous Cushing syndrome
The treatment is gradual glucocorticoid reduction when clinically safe. Steroids should not be stopped abruptly if the hypothalamic-pituitary-adrenal axis is suppressed.
Pituitary Cushing disease
First-line treatment is usually transsphenoidal pituitary surgery.
If disease persists or recurs, options may include repeat surgery, pituitary radiation, medical therapy, or bilateral adrenalectomy in refractory cases.
Adrenal Cushing syndrome
Adrenal adenomas or carcinomas are treated with adrenalectomy when appropriate.
Ectopic ACTH syndrome
The goal is to localize and resect the ACTH-producing tumor when feasible. If the tumor cannot be found or removed, medical cortisol-lowering therapy may be needed.
Medical therapy
Medical therapy may be used while awaiting surgery, after incomplete surgical response, while waiting for radiation to work, or when surgery is not possible.
Options include:
Steroidogenesis inhibitors such as ketoconazole, metyrapone, osilodrostat, or mitotane
Pituitary-directed therapy such as pasireotide or cabergoline in selected patients
Glucocorticoid receptor blockade such as mifepristone in selected cases
Comorbidities should be treated aggressively at the same time: hypertension, diabetes, hypokalemia, infection risk, osteoporosis, mood disease, and thromboembolic risk.
Follow-up and monitoring
After treatment, patients require close monitoring because cortisol levels may fall quickly and adrenal insufficiency can occur.
Follow-up should include:
Cortisol assessment after surgery or medical therapy
Monitoring for adrenal insufficiency symptoms
Blood pressure and glucose monitoring
Potassium and metabolic labs
Weight and symptom tracking
Bone health assessment
Cardiovascular risk reduction
Surveillance for recurrence
The 2015 Endocrine Society treatment guideline emphasizes that treatment should normalize cortisol levels or cortisol action and also address associated comorbidities. (PubMed)
Complications if untreated
Untreated Cushing syndrome carries major morbidity and mortality risk.
Important complications include:
Cardiovascular disease
Hypertension
Diabetes and dyslipidemia
Venous thromboembolism
Osteoporosis and fractures
Serious infections
Poor wound healing
Psychiatric morbidity
Muscle wasting and functional decline
The most important clinical point is that Cushing syndrome is not just a cosmetic or weight-gain disorder. It is a systemic disease with serious cardiometabolic, skeletal, infectious, and thrombotic consequences.
Clinical takeaway
Cushing syndrome should be suspected when a patient has progressive, clustered features of cortisol excess, especially central obesity with wide purple striae, proximal muscle weakness, easy bruising, resistant hypertension, diabetes, osteoporosis, or unexplained hypokalemia.
The practical approach is:
Exclude exogenous steroids.
Screen with late-night salivary cortisol, 24-hour urinary free cortisol, or dexamethasone suppression testing.
If hypercortisolism is confirmed, measure ACTH.
Localize the source.
Treat the cause and control cortisol-related complications.