The ATLANTIS trial, published in JAMA in 1999, evaluated whether intravenous recombinant tissue-type plasminogen activator, also known as rt-PA or alteplase, improves outcomes in patients with acute ischemic stroke when given 3 to 5 hours after symptom onset.
At the time, thrombolysis had already shown benefit when administered early after ischemic stroke. ATLANTIS asked an important question: could the treatment window be safely extended beyond 3 hours?
Trial Design
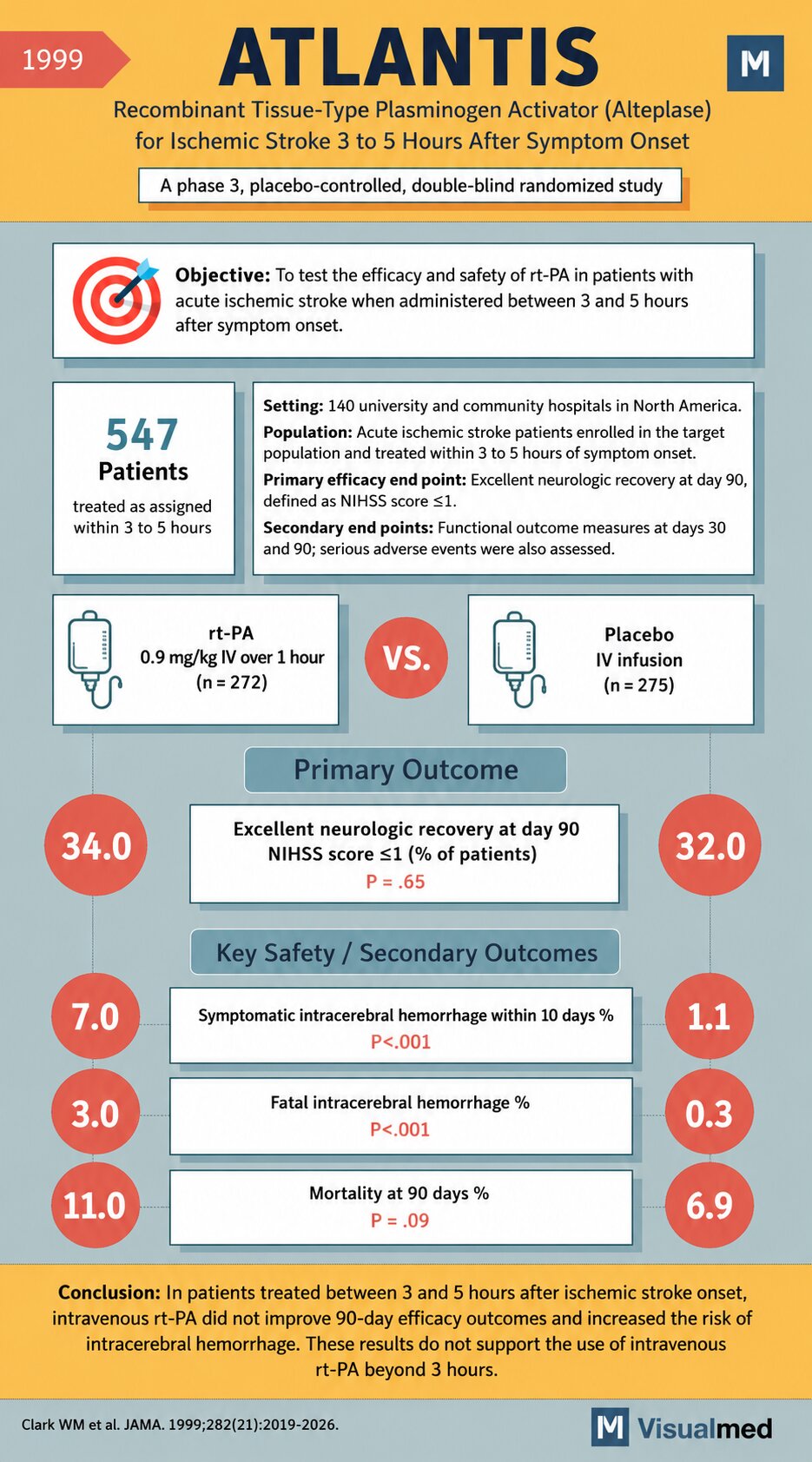
ATLANTIS was a phase 3, placebo-controlled, double-blind randomized trial conducted across 140 university and community hospitals in North America.
A total of 547 patients with acute ischemic stroke were enrolled in the target population and treated within 3 to 5 hours of symptom onset.
Patients were randomized to:
Alteplase group:
rt-PA 0.9 mg/kg IV over 1 hour
n = 272
Placebo group:
IV placebo infusion
n = 275
The primary efficacy endpoint was excellent neurologic recovery at 90 days, defined as a NIHSS score ≤1.
Secondary outcomes included functional outcome measures at days 30 and 90, along with serious adverse events.
Primary Outcome
ATLANTIS did not show a significant improvement in excellent neurologic recovery at 90 days.
Excellent neurologic recovery occurred in:
34.0% of patients in the rt-PA group
32.0% of patients in the placebo group
P = 0.65
This meant that alteplase, when given between 3 and 5 hours after stroke onset, did not significantly improve the main efficacy outcome compared with placebo.
Safety Outcomes
The major concern in ATLANTIS was bleeding risk.
Symptomatic intracerebral hemorrhage within 10 days occurred in:
7.0% with rt-PA
1.1% with placebo
P < 0.001
Fatal intracerebral hemorrhage occurred in:
3.0% with rt-PA
0.3% with placebo
P < 0.001
Mortality at 90 days was numerically higher with alteplase:
11.0% with rt-PA
6.9% with placebo
P = 0.09
Although the mortality difference did not reach statistical significance, the increase in symptomatic and fatal intracerebral hemorrhage was clinically important.
Clinical Interpretation
ATLANTIS demonstrated that, in patients treated 3 to 5 hours after ischemic stroke onset, alteplase did not improve 90-day neurologic outcomes and was associated with a significantly increased risk of intracerebral hemorrhage.
The trial therefore did not support routine use of IV rt-PA beyond 3 hours in the population studied.
Bottom Line
The ATLANTIS trial was an important negative trial in stroke thrombolysis. It showed that extending alteplase treatment to the 3-to-5-hour window without better patient selection did not improve outcomes and increased bleeding risk.
Reference:
Clark WM et al. JAMA. 1999;282(21):2019-2026.