Primary membranous nephropathy is an immune-mediated glomerular disease and a major cause of nephrotic syndrome in adults. Treatment often aims to reduce proteinuria, preserve kidney function, and achieve durable remission while minimizing drug toxicity. Calcineurin inhibitors such as tacrolimus can reduce proteinuria, but relapse and long-term kidney safety remain important concerns.
The MAJESTY Trial evaluated whether obinutuzumab, an intravenous type II anti-CD20 monoclonal antibody, could provide superior efficacy compared with oral tacrolimus in adults with primary membranous nephropathy.
Trial Design
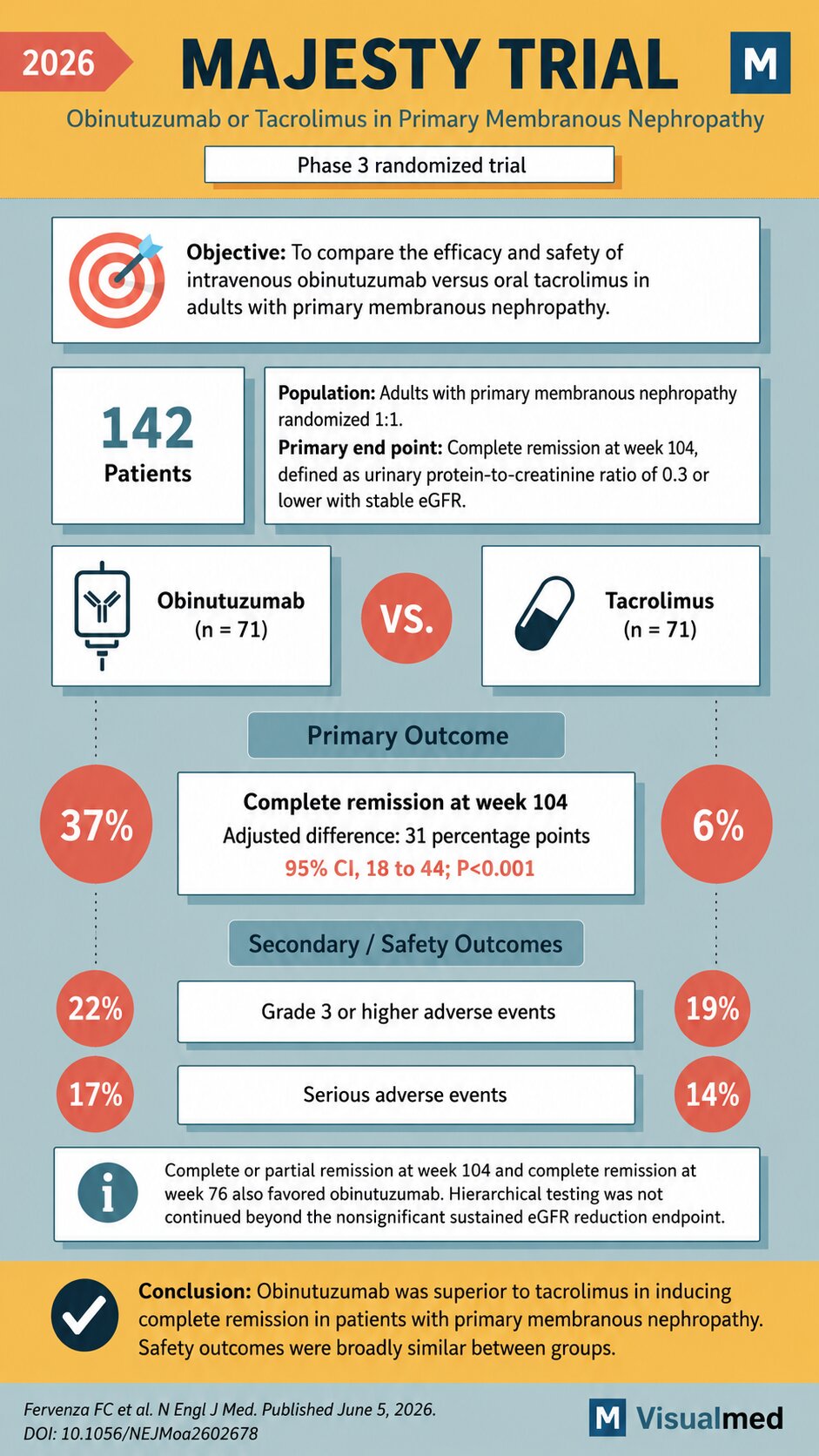
The MAJESTY trial was a phase 3 randomized trial including 142 adults with primary membranous nephropathy. Participants were randomized in a 1:1 fashion to receive either:
Obinutuzumab: 71 patients
Tacrolimus: 71 patients
The primary end point was complete remission at week 104, defined as a urinary protein-to-creatinine ratio of 0.3 or lower with stable estimated glomerular filtration rate.
Primary Outcome
Obinutuzumab demonstrated a clear benefit over tacrolimus for the primary end point.
At week 104, complete remission occurred in 37% of patients receiving obinutuzumab compared with 6% of patients receiving tacrolimus.
The adjusted difference was 31 percentage points, with a 95% confidence interval of 18 to 44, and the result was statistically significant with P<0.001.
This is a clinically important finding because complete remission in membranous nephropathy is strongly associated with improved long-term kidney outcomes and lower risk of disease progression.
Secondary and Safety Outcomes
Safety outcomes were broadly similar between groups.
Grade 3 or higher adverse events occurred in 22% of the obinutuzumab group and 19% of the tacrolimus group.
Serious adverse events occurred in 17% of the obinutuzumab group and 14% of the tacrolimus group.
The trial also reported that complete or partial remission at week 104 and complete remission at week 76 favored obinutuzumab. However, hierarchical testing was not continued beyond the nonsignificant sustained eGFR reduction end point.
Clinical Interpretation
The MAJESTY trial suggests that B-cell–targeted therapy with obinutuzumab may offer a stronger remission strategy than tacrolimus in primary membranous nephropathy.
The magnitude of benefit was substantial: complete remission was more than six times higher with obinutuzumab than tacrolimus at 104 weeks. Importantly, this occurred without a major apparent safety penalty based on the reported rates of serious or grade 3 or higher adverse events.
For clinicians, the trial supports obinutuzumab as a potentially important therapeutic option in primary membranous nephropathy, especially for patients in whom durable immunologic and proteinuric remission is the goal.
Bottom Line
In the MAJESTY trial, obinutuzumab was superior to tacrolimus in inducing complete remission among adults with primary membranous nephropathy. Safety outcomes were broadly similar between treatment groups.
Reference: Fervenza FC et al. New England Journal of Medicine. Published June 5, 2026. DOI: 10.1056/NEJMoa2602678.