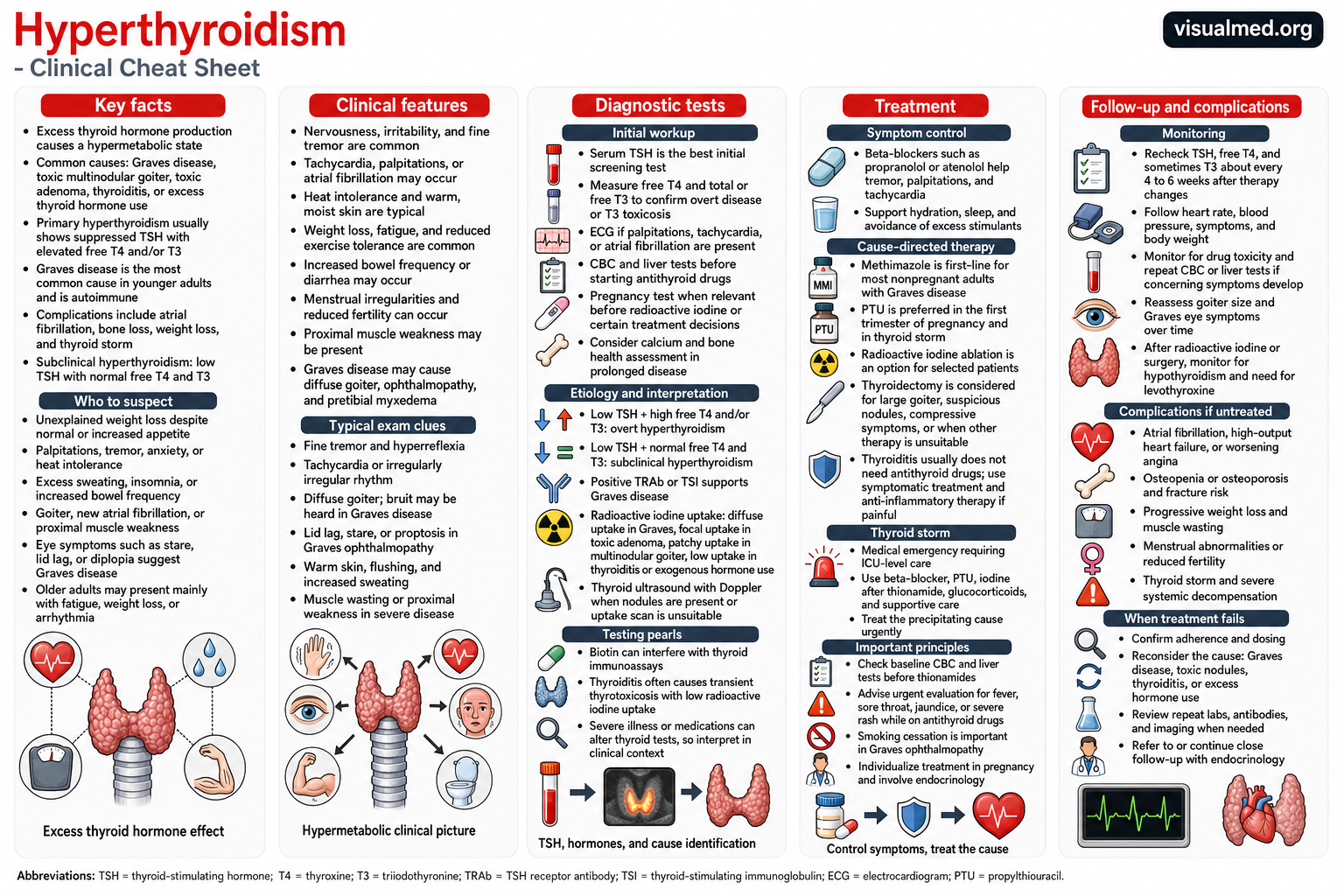
Hyperthyroidism is a condition in which the thyroid gland produces and releases excessive amounts of thyroid hormone. Because thyroid hormones influence energy use, body temperature, heart rate, digestion, muscle function, and many other processes, excess hormone creates a widespread hypermetabolic state in which many body systems speed up.
The condition is usually treatable, but untreated hyperthyroidism can lead to atrial fibrillation, heart failure, osteoporosis, severe muscle loss, and—in rare cases—a life-threatening thyroid storm.
Hyperthyroidism Versus Thyrotoxicosis
The terms are often used interchangeably, but they are not identical.
Thyrotoxicosis means that the body is exposed to excessive thyroid hormone from any source. Hyperthyroidism specifically refers to excessive synthesis and secretion of thyroid hormone by the thyroid gland.
For example, Graves disease and toxic thyroid nodules cause true hyperthyroidism. Thyroiditis can cause thyrotoxicosis when inflammation releases thyroid hormone that was already stored inside the gland, even though the gland is not actively producing more hormone.
What Causes Hyperthyroidism?
Graves Disease
Graves disease is the most common cause of hyperthyroidism in the United States. It is an autoimmune disorder in which antibodies stimulate the thyroid-stimulating hormone receptor, causing the entire thyroid gland to produce excessive hormone.
Graves disease may also cause a diffuse goiter, thyroid eye disease, and—less commonly—pretibial myxedema.
Toxic Adenoma
A toxic adenoma is a single thyroid nodule that produces thyroid hormone independently of normal pituitary regulation.
Toxic Multinodular Goiter
In toxic multinodular goiter, several autonomously functioning nodules produce excess hormone. This cause becomes more common with increasing age and in regions with lower dietary iodine intake.
Thyroiditis
Inflammation can cause stored thyroid hormone to leak into the bloodstream. Thyroiditis may be painless, painful following a viral illness, postpartum, medication-related, or associated with other inflammatory conditions.
Because the problem is hormone leakage rather than increased hormone synthesis, antithyroid medications are generally ineffective for thyroiditis. The thyrotoxic phase is often temporary, although some patients subsequently develop hypothyroidism.
Excess Thyroid Hormone or Iodine Exposure
Thyrotoxicosis can also result from taking too much prescribed thyroid hormone, using supplements that contain thyroid hormone, or exposure to iodine-containing medications such as amiodarone.
Common Symptoms
Symptoms vary considerably. Some patients develop an obvious hypermetabolic syndrome, while older adults may present only with fatigue, weight loss, depression, weakness, or an arrhythmia.
Common symptoms include:
- Unexplained weight loss despite a normal or increased appetite
- Palpitations or a rapid heartbeat
- Anxiety, nervousness, or irritability
- Fine hand tremor
- Heat intolerance and increased sweating
- Difficulty sleeping
- Frequent bowel movements or diarrhea
- Fatigue and reduced exercise tolerance
- Proximal muscle weakness
- Menstrual irregularities
- Hair thinning
- Neck swelling or difficulty swallowing
Thyroid hormone excess may also cause atrial fibrillation, particularly in older patients or those with underlying cardiovascular disease.
Physical Examination Findings
Possible examination findings include:
- Tachycardia or an irregularly irregular rhythm
- Fine tremor
- Hyperreflexia
- Warm, moist skin
- Muscle wasting
- Diffuse or nodular thyroid enlargement
- A thyroid bruit in Graves disease
- Lid lag or a prominent stare
- Proptosis or eye inflammation
- Lower-leg skin thickening in Graves disease
Eye disease is particularly suggestive of Graves disease and is not a typical feature of toxic nodules or thyroiditis.
How Is Hyperthyroidism Diagnosed?
Thyroid-Stimulating Hormone
Serum TSH is generally the best initial screening test. In primary hyperthyroidism, TSH is usually very low or undetectable because the pituitary gland is attempting to reduce thyroid hormone production.
Free T4 and T3
If TSH is suppressed, free T4 and total or free T3 should be measured.
Typical patterns include:
- Overt hyperthyroidism: low TSH with elevated free T4, T3, or both
- T3 toxicosis: low TSH with elevated T3 but normal free T4
- Subclinical hyperthyroidism: low TSH with normal free T4 and T3
Subclinical hyperthyroidism does not always require immediate treatment. Decisions depend on the degree and persistence of TSH suppression, the underlying cause, symptoms, age, and the presence of cardiovascular disease or osteoporosis.
Determining the Cause
Identifying the cause is essential because the appropriate treatment differs significantly between Graves disease, autonomous nodules, and thyroiditis.
Thyroid Antibodies
Positive TSH-receptor antibodies, including TRAb or thyroid-stimulating immunoglobulin, strongly support Graves disease. In many patients, a positive antibody test can establish the cause without further imaging.
Radioactive Iodine Uptake Scan
A radioactive iodine uptake scan shows how actively different parts of the thyroid absorb iodine.
Typical patterns include:
- Diffuse increased uptake in Graves disease
- Focal uptake in a toxic adenoma
- Patchy uptake in toxic multinodular goiter
- Low or nearly absent uptake in thyroiditis, recent iodine exposure, or excess thyroid-hormone ingestion
Radioactive iodine testing should not be performed during pregnancy or breastfeeding.
Thyroid Ultrasound
Ultrasound is particularly useful when thyroid nodules are present or when radioactive iodine testing is unsuitable. Doppler imaging may also demonstrate increased thyroid blood flow in Graves disease.
Treatment of Hyperthyroidism
Treatment depends on the cause, severity, age, pregnancy status, goiter size, eye disease, underlying medical conditions, and patient preference. The principal treatment strategies are symptom control, antithyroid medication, radioactive iodine, and surgery.
Beta-Blockers for Symptom Control
Beta-blockers such as propranolol, atenolol, or metoprolol can reduce palpitations, tachycardia, tremor, anxiety, and heat intolerance.
They can be started before the precise cause is known because they control the adrenergic effects of excess thyroid hormone. However, they do not correct the underlying thyroid disorder or directly normalize hormone production.
Antithyroid Medications
The two principal antithyroid medications are:
- Methimazole
- Propylthiouracil, or PTU
These medications reduce new thyroid-hormone synthesis and are effective in Graves disease and autonomous thyroid hormone production. They are not effective for destructive thyroiditis.
Methimazole is generally preferred for most nonpregnant adults because it has a more favorable safety profile and can often be taken less frequently. PTU is generally reserved for selected situations, including thyroid storm and the first trimester of pregnancy.
Important Adverse Effects
Antithyroid drugs can rarely cause severe liver injury or agranulocytosis, a dangerous reduction in infection-fighting white blood cells.
Patients taking methimazole or PTU should seek urgent medical advice if they develop:
- Fever
- Severe sore throat
- Jaundice
- Dark urine
- Significant abdominal pain
- A severe rash
The American Thyroid Association advises patients with fever or severe sore throat to stop further doses temporarily and obtain urgent evaluation with a blood count until a clinician determines whether treatment can safely resume.
Radioactive Iodine
Radioactive iodine is absorbed by active thyroid cells and gradually destroys the tissue producing excess hormone. It can be used for Graves disease, toxic adenoma, and toxic multinodular goiter, but it is ineffective for thyroiditis.
Its effect develops over several weeks to months. Many patients—particularly those treated for Graves disease—eventually develop permanent hypothyroidism and require lifelong levothyroxine. Radioactive iodine is contraindicated during pregnancy and breastfeeding and may worsen active thyroid eye disease in susceptible patients.
Thyroid Surgery
Thyroidectomy provides rapid and definitive control. It may be favored when a patient has:
- A very large goiter
- Compressive symptoms
- Suspicious or malignant nodules
- Significant thyroid eye disease
- A need for rapid definitive treatment
- Medication intolerance
- Hyperthyroidism that has not responded to other treatment
- A preference to avoid radioactive iodine
Patients should generally be rendered euthyroid before elective surgery. Total thyroidectomy results in permanent hypothyroidism and therefore requires lifelong thyroid-hormone replacement. Surgery should preferably be performed by an experienced, high-volume thyroid surgeon.
Treatment of Thyroiditis
Because thyroiditis causes the release of stored hormone rather than increased synthesis, methimazole and PTU usually do not help.
Treatment may include:
- Beta-blockers for palpitations or tremor
- Nonsteroidal anti-inflammatory medication for pain
- Corticosteroids in more severe painful thyroiditis
- Temporary thyroid-hormone replacement if a significant hypothyroid phase develops
Hyperthyroidism During Pregnancy
Hyperthyroidism during pregnancy requires careful coordination between endocrinology and obstetric or maternal-fetal medicine specialists.
The 2026 American Thyroid Association guideline states that PTU is preferred over methimazole during the first trimester when antithyroid therapy is required. After approximately 16 weeks, the choice of medication should be individualized because both drugs have potential maternal and fetal risks. Radioactive iodine must not be used during pregnancy.
Thyroid Storm
Thyroid storm is a rare but life-threatening form of severe thyrotoxicosis with systemic decompensation. Features may include:
- High fever
- Severe tachycardia or atrial fibrillation
- Heart failure
- Agitation, delirium, or coma
- Vomiting or diarrhea
- Liver dysfunction
- Hypotension or shock
It requires immediate intensive-care treatment. Management generally combines beta-blockade, an antithyroid medication, iodine administered after the antithyroid drug, corticosteroids, cooling, intravenous fluids, respiratory and nutritional support, and urgent treatment of the precipitating illness.
Follow-Up and Monitoring
Patients starting antithyroid therapy typically have free T4 and T3 reassessed within approximately two to six weeks. Testing is repeated after dose changes, while recognizing that TSH may remain suppressed for several months even after hormone levels begin to normalize.
After radioactive iodine or thyroidectomy, continued testing is required to detect hypothyroidism and begin or adjust levothyroxine. Patients should also be monitored for recurrent symptoms, heart rhythm abnormalities, changes in body weight, bone health, goiter size, and progression of thyroid eye disease.
Potential Complications
Untreated or inadequately controlled hyperthyroidism may cause:
- Atrial fibrillation
- Embolic stroke related to atrial fibrillation
- Worsening angina
- High-output heart failure
- Osteopenia or osteoporosis
- Fractures
- Progressive muscle wasting
- Menstrual and fertility problems
- Severe weight loss
- Thyroid storm
The cardiovascular effects are particularly important in older adults and patients with pre-existing heart disease.
Key Takeaway
Hyperthyroidism should be considered in patients with unexplained weight loss, palpitations, tremor, heat intolerance, sweating, goiter, atrial fibrillation, or proximal muscle weakness.
A suppressed TSH followed by measurement of free T4 and T3 establishes the biochemical diagnosis. Antibody testing, radioactive iodine uptake, and ultrasound help determine the underlying cause.
Treatment must then be tailored to that cause. Beta-blockers control symptoms, antithyroid medications suppress new hormone production, and radioactive iodine or surgery can provide definitive treatment. Prompt diagnosis and appropriate follow-up can prevent most serious cardiovascular, skeletal, and systemic complications.
This article is intended for medical education and does not replace individualized evaluation or treatment by a qualified healthcare professional.