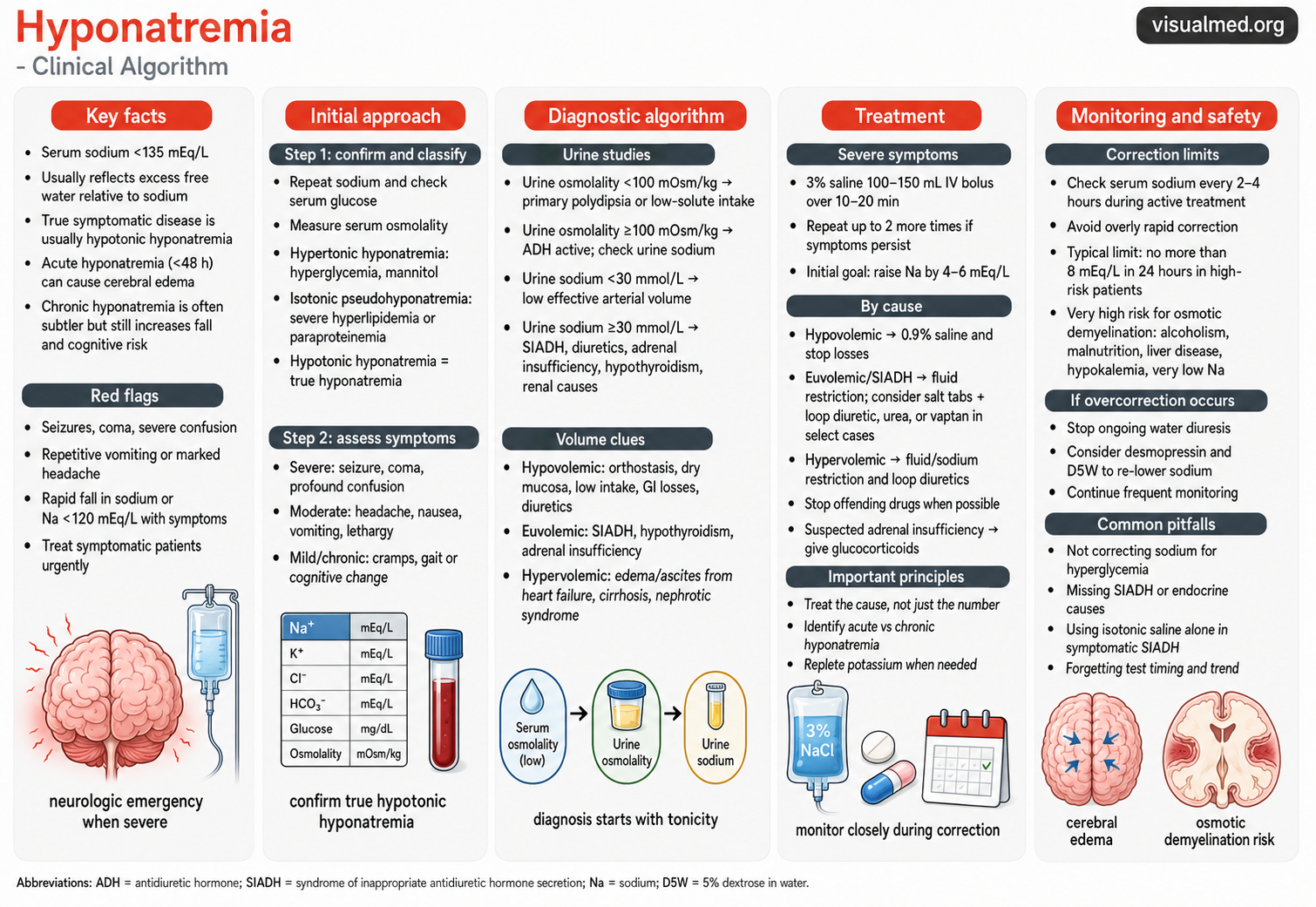
Hyponatremia is usually defined as a serum sodium concentration below 135 mEq/L and is one of the most common electrolyte abnormalities encountered in clinical practice. The key concept is that hyponatremia usually reflects excess water relative to sodium, not simply a “sodium deficiency.” The danger is not just the number itself, but the speed of onset, symptom severity, and risk of cerebral edema or osmotic demyelination during correction.
Start with the patient, not the sodium number
The first question is whether the patient has severe neurologic symptoms. Seizures, coma, profound confusion, severe lethargy, or signs of increased intracranial pressure should be treated as a medical emergency. Acute hyponatremia, especially when it develops over less than 48 hours, can cause cerebral edema because water shifts into brain cells. Chronic hyponatremia may look more subtle but is still clinically important because it can contribute to gait instability, falls, cognitive changes, and frailty.
For severe symptomatic hyponatremia, consensus guidance supports urgent treatment with 3% hypertonic saline, commonly as a 100–150 mL IV bolus, with repeat boluses if severe symptoms persist. The early goal is not to normalize sodium; it is to raise serum sodium enough to reduce life-threatening cerebral edema, often by about 4–6 mEq/L.
Step 1: Confirm true hypotonic hyponatremia
Once the patient is stabilized, confirm that the hyponatremia is truly hypotonic. This matters because not all low sodium values represent the same physiology.
Check:
- Repeat serum sodium
- Serum glucose
- Serum osmolality
- Basic metabolic panel
- Medication list
- Recent fluids, diuretics, vomiting, diarrhea, surgery, pain, nausea, or CNS/pulmonary disease
Hyperglycemia can cause translocational hyponatremia. Severe hyperlipidemia or paraproteinemia can cause pseudohyponatremia. The classic diagnostic approach starts with serum tonicity/osmolality, because patients with normal or elevated effective osmolality should not be managed the same way as patients with true hypotonic hyponatremia.
Step 2: Use urine osmolality to decide whether ADH is active
In true hypotonic hyponatremia, the next key test is urine osmolality.
If urine osmolality is <100 mOsm/kg, the kidney is appropriately producing dilute urine. This pattern suggests excess water intake relative to solute, such as primary polydipsia, low-solute intake, or “tea and toast” physiology.
If urine osmolality is ≥100 mOsm/kg, antidiuretic hormone activity is present. That means the kidney is not freely excreting water, and the differential shifts toward SIADH, hypovolemia, adrenal insufficiency, hypothyroidism, diuretics, renal failure, heart failure, cirrhosis, or nephrotic syndrome. Hypotonic hyponatremia is commonly differentiated using urine osmolality, urine sodium, and clinical volume status.
Step 3: Use urine sodium and volume status
After urine osmolality, check urine sodium.
A urine sodium <30 mmol/L usually suggests low effective arterial blood volume. This may occur with true hypovolemia from vomiting, diarrhea, poor intake, or third spacing. It can also occur in hypervolemic states such as heart failure or cirrhosis, where total body water is high but effective arterial volume is low.
A urine sodium ≥30 mmol/L suggests that the kidney is not avidly retaining sodium. This pattern can be seen with SIADH, adrenal insufficiency, hypothyroidism, renal salt wasting, kidney disease, or diuretic use.
Volume status then helps separate the major categories:
Hypovolemic hyponatremia: orthostasis, dry mucosa, low intake, vomiting, diarrhea, diuretic use.
Euvolemic hyponatremia: SIADH, hypothyroidism, adrenal insufficiency, medication effect.
Hypervolemic hyponatremia: edema or ascites from heart failure, cirrhosis, nephrotic syndrome, or advanced kidney disease.
Treatment depends on symptoms and cause
For severe symptomatic hyponatremia, treat immediately with hypertonic saline and close monitoring.
For hypovolemic hyponatremia, treatment is usually isotonic saline and correction of ongoing losses. As volume is restored, ADH can shut off and the sodium may rise quickly, so monitoring urine output and serum sodium is critical.
For euvolemic hyponatremia/SIADH, initial therapy often includes fluid restriction. Depending on the clinical context, additional options may include increased solute intake, salt tablets with loop diuretics, oral urea, or selected use of vasopressin antagonists. Vaptans should not be used routinely in all patients and require careful monitoring.
For hypervolemic hyponatremia, treatment usually focuses on fluid and sodium restriction, loop diuretics, and management of the underlying condition, such as heart failure, cirrhosis, or nephrotic syndrome.
If adrenal insufficiency is suspected, do not miss it. Hyponatremia may improve rapidly after glucocorticoid replacement, so these patients also require careful monitoring for overcorrection.
Correction limits: avoid causing harm
The major danger during treatment is correcting chronic hyponatremia too quickly, which can cause osmotic demyelination syndrome. Patients at especially high risk include those with very low sodium, alcoholism, malnutrition, liver disease, hypokalemia, or other severe chronic illness.
Modern expert guidance generally emphasizes conservative correction. In high-risk patients, correction should not exceed 8 mmol/L in any 24-hour period. Some guidance allows higher limits in lower-risk patients, but many clinicians aim for a safer target of roughly 4–8 mEq/L per day, especially when chronicity is uncertain.
During active correction, serum sodium should be checked frequently, often every 2–4 hours in severe cases or when using hypertonic saline. If sodium begins rising too quickly, clinicians may need to stop the ongoing water diuresis and consider desmopressin with D5W to re-lower or stabilize serum sodium. Desmopressin has been used to prevent or reverse inadvertent overcorrection in severe hyponatremia.
Common pitfalls
The biggest mistake is treating the sodium number without understanding the physiology. Other common errors include failing to correct sodium for hyperglycemia, missing SIADH or endocrine causes, using isotonic saline alone in symptomatic SIADH, ignoring potassium repletion, and forgetting that sodium can rise rapidly once ADH turns off.
Another important pitfall is forgetting that the initial goal in severe symptomatic hyponatremia is partial correction, not normalization. Once the neurologic emergency is controlled, the priority shifts to slow, safe, cause-directed correction.
Clinical bottom line
Hyponatremia management starts with symptoms, then tonicity, then urine studies. Severe neurologic symptoms require urgent hypertonic saline. Stable patients require a structured approach using serum osmolality, urine osmolality, urine sodium, and volume status. The safest clinicians treat the cause, monitor closely, and respect correction limits.