Wide-complex tachycardia is one of the most important ECG patterns to recognize quickly. The key clinical question is simple: is this ventricular tachycardia, or is it supraventricular tachycardia with aberrant conduction?
In practice, the safest rule is this: a regular wide-complex tachycardia should be treated as VT until proven otherwise, especially in an older patient or someone with known structural heart disease. Several ECG clues can help distinguish VT from SVT with aberrancy.
Why This Distinction Matters
Both VT and SVT with aberration can present as a fast, wide QRS rhythm. However, the implications are very different.
Ventricular tachycardia originates from the ventricles and may deteriorate into hemodynamic instability or cardiac arrest. SVT with aberration begins above the ventricles but conducts with a bundle branch block pattern, making the QRS appear wide.
The ECG diagnosis is not always obvious, but certain findings strongly favor VT.
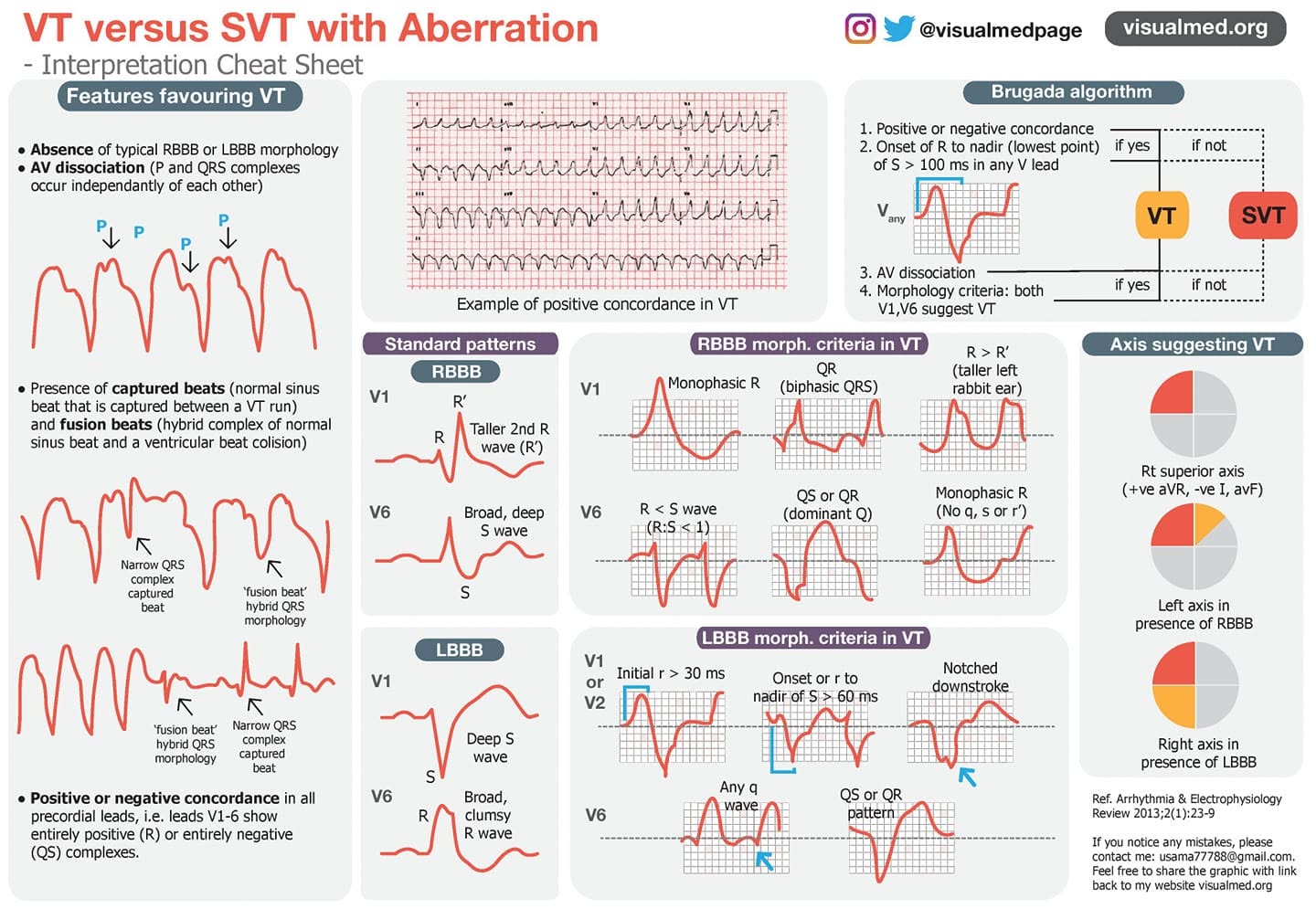
Key ECG Features Favoring VT
1. Absence of Typical RBBB or LBBB Morphology
SVT with aberrancy usually follows a recognizable bundle branch block pattern: either typical right bundle branch block or typical left bundle branch block.
When the QRS morphology does not resemble a typical RBBB or LBBB pattern, VT becomes more likely.
In other words, if the rhythm is wide and fast but the QRS shape looks “wrong” for standard bundle branch block, think VT.
2. AV Dissociation
One of the strongest clues for VT is AV dissociation.
This means the atria and ventricles are beating independently. On the ECG, you may see P waves marching through at their own rate, unrelated to the QRS complexes.
AV dissociation occurs because the ventricles are being driven by a ventricular rhythm, while the sinus node continues to activate the atria separately.
When present, AV dissociation is highly suggestive of VT.
3. Capture Beats and Fusion Beats
Two classic findings that support VT are capture beats and fusion beats.
A capture beat occurs when a normal sinus impulse briefly “captures” the ventricles during VT, producing a narrow QRS complex within the run of wide-complex tachycardia.
A fusion beat occurs when a sinus beat and a ventricular beat activate the ventricles at the same time, creating a hybrid QRS morphology.
Both findings imply that the atria and ventricles are not linked normally, which strongly favors VT.
4. Positive or Negative Concordance
Another important clue is precordial concordance.
This means all the chest leads, V1 through V6, point in the same direction.
Positive concordance means all precordial leads show predominantly positive QRS complexes.
Negative concordance means all precordial leads show predominantly negative QS complexes.
Either pattern is unusual for ordinary SVT with bundle branch block and strongly suggests VT.
The Brugada Algorithm
The Brugada algorithm is a structured approach to wide-complex tachycardia.
It asks several stepwise questions:
Step 1: Is there positive or negative concordance?
If yes, VT is favored.
Step 2: Is the RS interval greater than 100 ms in any precordial lead?
The RS interval is measured from the onset of the R wave to the deepest point of the S wave. If this interval is greater than 100 ms, VT is favored.
Step 3: Is there AV dissociation?
If AV dissociation is present, VT is favored.
Step 4: Do morphology criteria suggest VT?
If the QRS pattern does not fit typical RBBB or LBBB aberrancy, VT is more likely.
RBBB Morphology: What Suggests VT?
When the wide-complex rhythm has an RBBB-like pattern, certain ECG findings support VT.
In V1, VT is suggested by:
- A monophasic R wave
- A QR pattern
- A taller left rabbit ear, where the first R wave is taller than the second R′ wave
In V6, VT is suggested by:
- R wave smaller than S wave
- QS or QR pattern
- Monophasic R wave without the expected normal q, S, or r′ morphology
These findings are not typical for simple RBBB aberrancy and should raise suspicion for VT.
LBBB Morphology: What Suggests VT?
When the rhythm has an LBBB-like pattern, VT is suggested by specific features in V1, V2, and V6.
In V1 or V2, findings favoring VT include:
- Initial r wave duration greater than 30 ms
- Time from QRS onset to the nadir of the S wave greater than 60 ms
- Notching on the downstroke of the S wave
In V6, VT is suggested by:
- Any q wave
- QS or QR pattern
These features indicate abnormal ventricular activation rather than typical supraventricular conduction with LBBB aberrancy.
Axis Clues Suggesting VT
The frontal plane axis can also provide helpful clues.
Patterns that favor VT include:
- Superior axis
- Left axis deviation in the presence of RBBB morphology
- Right axis deviation in the presence of LBBB morphology
Axis alone should not be used to make the diagnosis, but when combined with morphology, AV dissociation, capture beats, or concordance, it can strongly support VT.
Practical Approach
When looking at a wide-complex tachycardia, ask yourself:
- Is the patient unstable?
- Is the rhythm regular or irregular?
- Does the QRS morphology fit typical RBBB or LBBB?
- Is there AV dissociation?
- Are capture or fusion beats present?
- Is there precordial concordance?
- Does the axis make sense for simple aberrancy?
If the answer is uncertain, it is safer to assume VT.
Key Takeaway
VT and SVT with aberration can look very similar, but several ECG findings strongly favor VT: AV dissociation, capture beats, fusion beats, concordance, atypical bundle branch morphology, and extreme or unexpected axis deviation.
The most important clinical principle is this:
When in doubt, treat wide-complex tachycardia as VT until proven otherwise.