Ventricular tachycardia (VT) is one of the most important arrhythmias to recognize on ECG. It is a potentially life-threatening rhythm that originates from the ventricles and can rapidly lead to hemodynamic collapse, cardiac arrest, or degeneration into ventricular fibrillation.
Because VT often presents as a wide-complex tachycardia, prompt recognition is critical. This cheat sheet highlights the key ECG features, common subtypes, diagnostic clues, underlying causes, and basic management principles of VT.
What Is Ventricular Tachycardia?
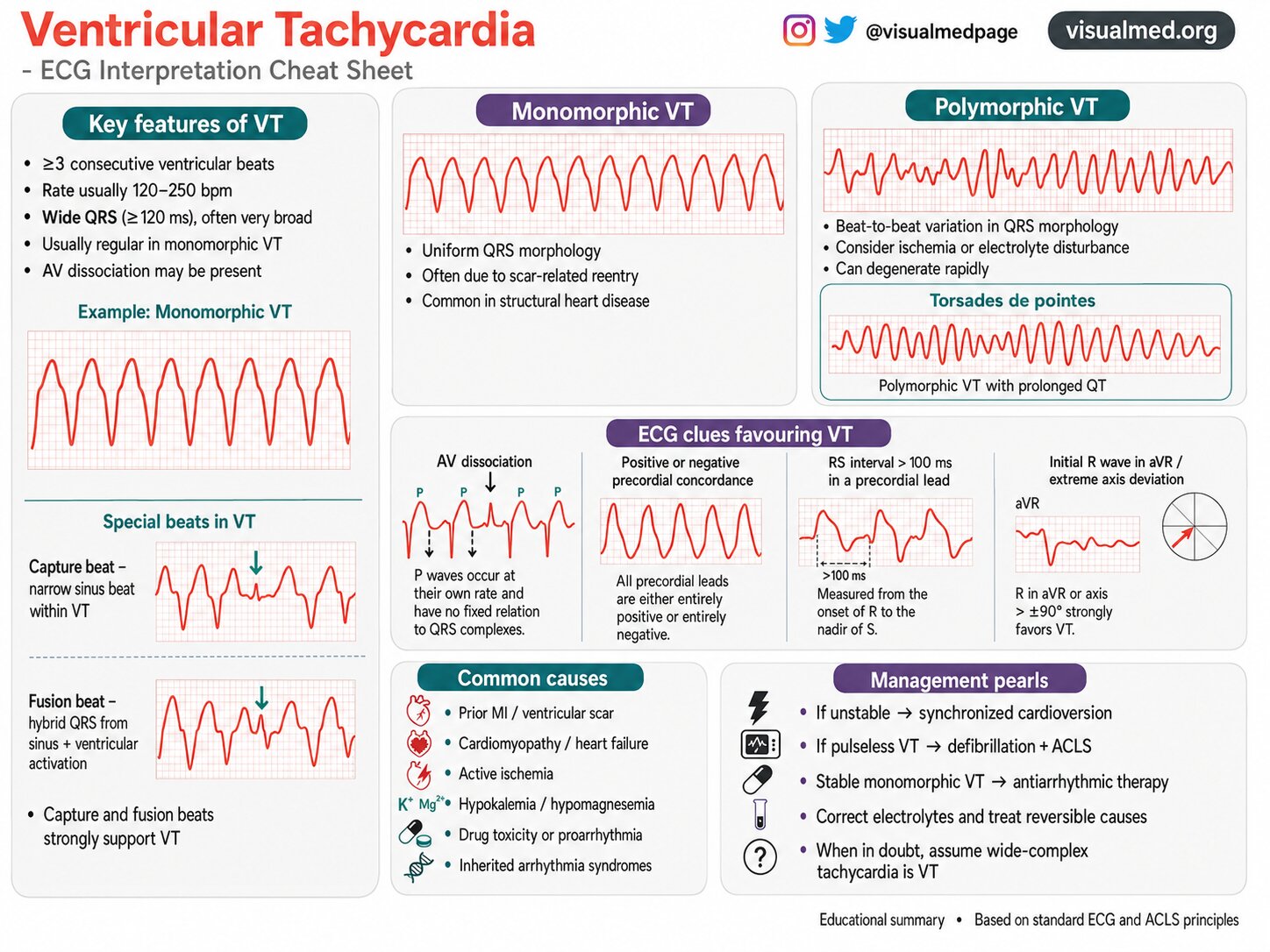
Ventricular tachycardia is defined as three or more consecutive ventricular beats occurring at a rapid rate, usually between 120 and 250 beats per minute. The rhythm typically produces a wide QRS complex (≥120 ms) because activation begins within the ventricles rather than through the normal His-Purkinje conduction system.
VT may be:
- Monomorphic, where each QRS complex has a similar shape
- Polymorphic, where the QRS morphology changes beat to beat
The distinction matters because it can suggest different underlying mechanisms and guide treatment.
Key ECG Features of VT
Several ECG findings strongly support the diagnosis of ventricular tachycardia:
- ≥3 consecutive ventricular beats
- Fast ventricular rate, usually 120–250 bpm
- Wide QRS complex, often very broad
- Usually regular rhythm in monomorphic VT
- AV dissociation may be present
In clinical practice, any regular wide-complex tachycardia should be presumed VT until proven otherwise, especially in patients with structural heart disease, prior myocardial infarction, or cardiomyopathy.
Monomorphic Ventricular Tachycardia
Monomorphic VT is the most common form of sustained VT. On the ECG, the QRS complexes appear uniform in shape from beat to beat.
Common characteristics:
- Uniform QRS morphology
- Usually regular rhythm
- Often caused by scar-related reentry
- Common in patients with prior MI or structural heart disease
This form of VT is often seen in patients with ventricular scar tissue, where abnormal reentry circuits develop and drive the tachycardia.
Polymorphic Ventricular Tachycardia
Polymorphic VT has a changing QRS morphology, meaning the appearance of the QRS varies from beat to beat.
Important features:
- Beat-to-beat variation in QRS shape
- Often associated with ischemia
- Can also occur with electrolyte abnormalities
- May degenerate quickly into ventricular fibrillation
Because polymorphic VT is generally more unstable, rapid identification and treatment are essential.
Torsades de Pointes
A special type of polymorphic VT is torsades de pointes, classically associated with a prolonged QT interval.
ECG appearance:
- QRS complexes appear to “twist” around the baseline
- Waxing and waning amplitude
- Irregular polymorphic ventricular rhythm
Common triggers:
- QT-prolonging medications
- Hypokalemia
- Hypomagnesemia
- Congenital long QT syndromes
Torsades is a medical emergency because it can quickly deteriorate into ventricular fibrillation.
Special Beats That Strongly Support VT
Two classic ECG findings that strongly favor VT are capture beats and fusion beats.
Capture Beat
A capture beat occurs when a sinus impulse transiently conducts to the ventricles during VT, producing a narrower, more normal-looking QRS complex in the middle of wide-complex tachycardia.
Fusion Beat
A fusion beat occurs when a sinus beat and a ventricular beat activate the ventricles simultaneously, creating a hybrid QRS morphology that looks intermediate between the two.
Both findings are highly supportive of VT because they indicate that the rhythm originates in the ventricles rather than being a supraventricular rhythm with aberrancy.
ECG Clues Favoring VT
When evaluating a wide-complex tachycardia, several clues can help identify VT.
1. AV Dissociation
AV dissociation means the atria and ventricles are depolarizing independently.
On ECG:
- P waves may be present
- P waves march through at their own rate
- There is no fixed relationship between P waves and QRS complexes
This is one of the strongest clues favoring VT.
2. Positive or Negative Concordance
Concordance refers to all precordial leads showing QRS complexes in the same direction.
- Positive concordance: all precordial leads are predominantly positive
- Negative concordance: all precordial leads are predominantly negative
Either pattern strongly favors VT.
3. RS Interval > 100 ms
If the interval from the onset of the R wave to the nadir of the S wave is greater than 100 ms in a precordial lead, VT is more likely.
This suggests abnormal ventricular activation rather than normal supraventricular conduction with bundle branch block.
4. Initial R Wave in aVR or Extreme Axis Deviation
Certain axis findings are also helpful.
Features that support VT include:
- Initial R wave in aVR
- Extreme axis deviation
- QRS axis beyond ±90°
These findings reflect ventricular-origin activation and should raise suspicion for VT.
Common Causes of Ventricular Tachycardia
VT is often a marker of underlying cardiac disease, though metabolic and inherited causes may also play a role.
Common causes include:
- Prior myocardial infarction with ventricular scar
- Cardiomyopathy
- Heart failure
- Active ischemia
- Hypokalemia
- Hypomagnesemia
- Drug toxicity or proarrhythmia
- Inherited arrhythmia syndromes
Identifying and treating the underlying cause is just as important as treating the rhythm itself.
Why VT Matters Clinically
VT can range from relatively tolerated to immediately life-threatening.
Possible consequences include:
- Hypotension
- Syncope
- Chest pain
- Heart failure
- Cardiac arrest
- Degeneration to ventricular fibrillation
The clinical context matters. A patient with VT who is unstable requires urgent intervention.
Management Pearls
Management depends largely on whether the patient is stable or unstable.
If the patient is unstable:
Perform synchronized cardioversion.
Signs of instability may include:
- Hypotension
- Altered mental status
- Ongoing chest pain
- Signs of shock
- Acute heart failure
If the patient has pulseless VT:
Treat with defibrillation and ACLS protocol.
If the patient has stable monomorphic VT:
Consider antiarrhythmic therapy, depending on the situation and clinical setting.
Additional key steps:
- Correct electrolytes
- Treat reversible causes
- Evaluate for ischemia
- Review medications for proarrhythmic agents
And one of the most important bedside principles:
When in doubt, assume a wide-complex tachycardia is VT.
Practical Takeaway
Ventricular tachycardia is a rhythm every clinician should recognize quickly. The combination of a wide-complex tachycardia, AV dissociation, capture or fusion beats, concordance, prolonged RS interval, and extreme axis deviation strongly points toward VT.
Understanding the difference between monomorphic VT, polymorphic VT, and torsades de pointes can help guide evaluation and treatment.
Prompt diagnosis saves lives.
Conclusion
VT is more than just a fast wide rhythm on ECG — it is often a sign of serious electrical and structural heart disease. A systematic ECG approach can make diagnosis easier and improve clinical decision-making.
Whether you are a student learning arrhythmias or a clinician reviewing emergency ECGs, remembering the major features of VT is essential:
- Wide QRS
- Ventricular origin
- AV dissociation
- Capture/fusion beats
- Concordance
- Important hemodynamic consequences
If you are faced with a wide-complex tachycardia and you are unsure, the safest approach is simple:
Treat it as VT until proven otherwise.