The ORBITA trial was a landmark study in interventional cardiology because it tested whether percutaneous coronary intervention, or PCI, improves symptoms in patients with stable angina when compared with a placebo procedure. Unlike many earlier PCI studies, the ORBITA trial used a double-blind sham-controlled design, making it one of the most rigorous trials ever performed in stable angina.
The key finding was surprising: in patients with stable angina and single-vessel coronary artery disease, PCI did not significantly improve treadmill exercise time compared with a sham PCI procedure after both groups received anti-anginal medical therapy.
Background: Why Was the ORBITA Trial Important?
PCI is commonly used to relieve angina in patients with obstructive coronary artery disease. While PCI clearly improves outcomes in acute coronary syndromes, its role in stable angina has always been more nuanced.
Before the ORBITA trial, many physicians believed that opening a significant coronary stenosis would predictably improve symptoms and exercise capacity. However, symptom improvement after a procedure can be influenced by placebo effect, patient expectations, medication optimization, and close follow-up.
The ORBITA trial was designed to isolate the true physiological and symptomatic effect of PCI by comparing it against a sham procedure.
Study Design
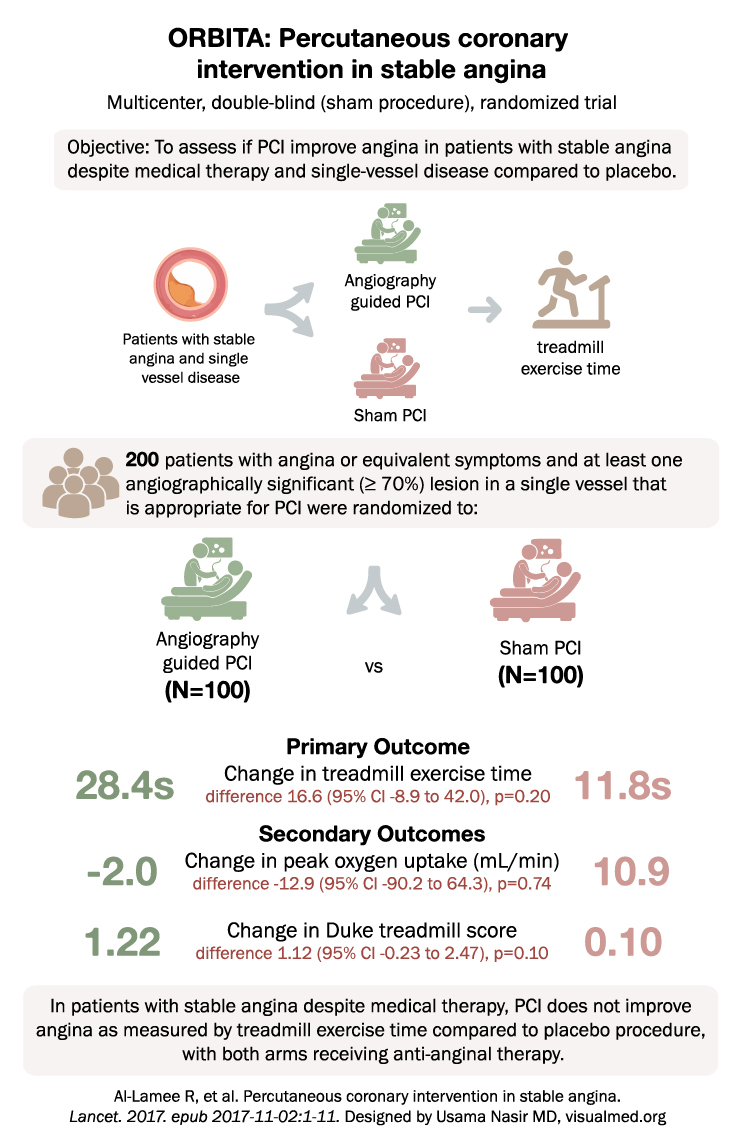
The ORBITA trial was a multicenter, double-blind, randomized controlled trial published in The Lancet in 2017.
The study enrolled 200 patients with stable angina or angina-equivalent symptoms. Patients had at least one angiographically significant lesion of 70% or greater in a single coronary vessel that was considered suitable for PCI.
Before randomization, patients underwent medical optimization. They were then randomized to:
- Angiography-guided PCI
- Sham PCI procedure
Both patients and assessing clinicians were blinded to treatment assignment.
Primary Outcome
The primary outcome of the ORBITA trial was:
Change in treadmill exercise time
The results were:
- PCI group: 28.4 seconds improvement
- Sham procedure group: 11.8 seconds improvement
The difference between groups was 16.6 seconds, with a 95% confidence interval from -8.9 to 42.0 seconds and a P value of 0.20.
This means PCI did not produce a statistically significant improvement in treadmill exercise time compared with the sham procedure.
Secondary Outcomes
The ORBITA trial also evaluated several secondary outcomes.
Change in Peak Oxygen Uptake
- PCI group: -2.0 mL/min
- Sham group: 10.9 mL/min
The difference was not statistically significant.
Change in Duke Treadmill Score
- PCI group: 1.22
- Sham group: 0.10
The difference was also not statistically significant.
Main Finding of the ORBITA Trial
The main message of the ORBITA trial was:
In patients with stable angina despite medical therapy, PCI did not significantly improve exercise time compared with a placebo procedure when both groups received anti-anginal therapy.
This was an important finding because it showed that the symptomatic benefit of PCI in stable angina may be smaller than previously assumed, especially after careful medical optimization.
Clinical Interpretation
The ORBITA trial does not mean PCI has no role in stable angina. PCI can still be useful in selected patients, especially those with persistent symptoms despite optimal medical therapy or high-risk anatomy. However, ORBITA challenged the assumption that PCI automatically produces major symptom improvement in all stable angina patients.
The study emphasized the importance of:
- Optimizing anti-anginal therapy before PCI
- Discussing realistic expectations with patients
- Recognizing the placebo effect in procedural medicine
- Using careful patient selection for invasive treatment
- Considering objective ischemia and symptom burden when making decisions
Why the ORBITA Trial Was Controversial
The ORBITA trial generated major debate because it questioned a common practice pattern in stable coronary disease. Some clinicians argued that the trial was small and had short follow-up. Others pointed out that it included patients with single-vessel disease and may not apply to patients with more extensive disease or severe refractory angina.
However, the trial’s sham-controlled design made it extremely important. It showed that in stable angina, symptom improvement after PCI must be interpreted carefully because placebo effect and medication optimization can contribute substantially.
ORBITA Trial and Stable Coronary Disease
The ORBITA trial fits into a broader body of evidence from trials such as COURAGE and ISCHEMIA. Together, these studies support a more conservative initial approach in many patients with stable coronary artery disease, especially when symptoms are manageable and there is no high-risk clinical presentation.
The practical takeaway is not that PCI should be abandoned. Rather, PCI should be used thoughtfully, with clear goals, especially when the goal is symptom relief rather than prevention of death or myocardial infarction.
Conclusion
The ORBITA trial showed that in patients with stable angina and single-vessel coronary artery disease, PCI did not significantly improve treadmill exercise time compared with a sham procedure after both groups received anti-anginal medical therapy.
This trial remains one of the most important studies in stable angina because it highlighted the power of placebo-controlled procedural trials and reinforced the need for optimal medical therapy before PCI.