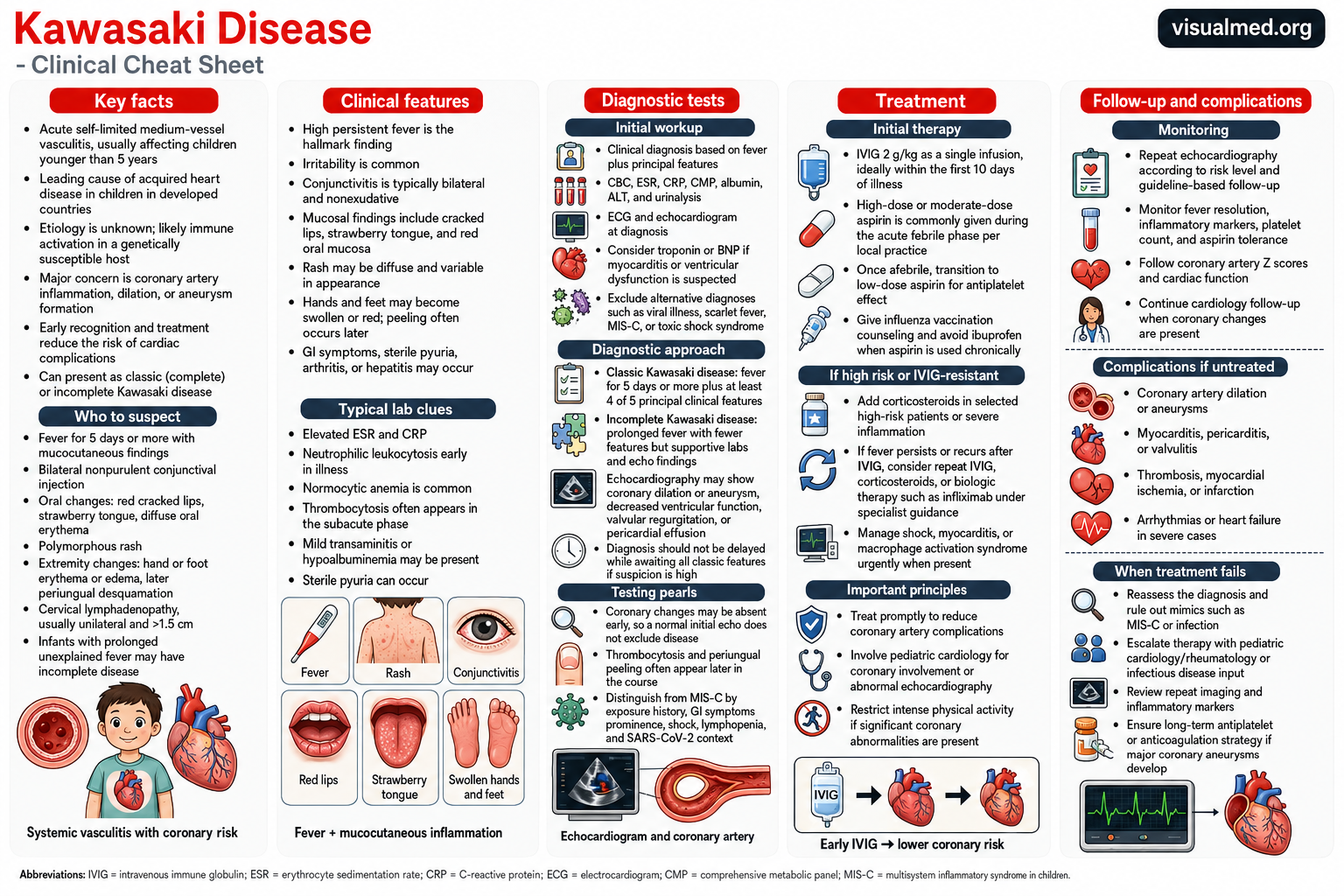
Kawasaki disease is an acute inflammatory illness that primarily affects infants and young children. It causes inflammation of medium-sized blood vessels throughout the body, with the coronary arteries being the most clinically important vessels involved.
Most cases occur in children younger than five years. Kawasaki disease is a leading cause of acquired heart disease in children because untreated inflammation can produce coronary artery dilation and aneurysms. Prompt recognition and treatment dramatically reduce this risk.
What Causes Kawasaki Disease?
The exact cause of Kawasaki disease remains unknown. Current evidence suggests that an environmental or infectious trigger may provoke an abnormal immune response in a genetically susceptible child. However, no single virus, bacterium, toxin, or environmental exposure has been proven to cause the disease.
Kawasaki disease is not considered contagious, and it does not usually spread between children.
Why Kawasaki Disease Matters
The most serious complication is inflammation of the coronary arteries—the blood vessels that supply oxygen to the heart muscle. Without treatment, approximately one-quarter of affected children may develop coronary artery dilation or aneurysms. Prompt treatment with intravenous immunoglobulin can reduce the risk to below 5%.
Coronary aneurysms can later become sites of:
- Blood-clot formation
- Progressive arterial narrowing
- Myocardial ischemia
- Myocardial infarction
- Arrhythmias or ventricular dysfunction
Although most children recover completely, patients who develop significant coronary abnormalities may require lifelong cardiology follow-up.
Classic Clinical Features
Persistent fever is the hallmark of Kawasaki disease. The traditional clinical diagnosis of complete Kawasaki disease is based on fever lasting at least five days together with at least four of five principal clinical features.
1. Bilateral conjunctival injection
The eyes appear red because of inflammation of the conjunctiva. The redness is usually bilateral and does not produce the thick purulent discharge typically associated with bacterial conjunctivitis.
2. Oral and mucosal changes
Common findings include:
- Bright red or cracked lips
- Diffuse redness of the mouth and throat
- A red, bumpy “strawberry tongue”
Oral ulcers and focal exudates are less typical and should prompt consideration of alternative diagnoses.
3. Polymorphous rash
The rash may appear on the trunk, extremities, or diaper area and can have several different appearances. Vesicles and bullae are not typical features.
4. Changes of the hands and feet
During the acute phase, the palms and soles may become red, painful, or swollen. During the second or third week, peeling commonly develops around the fingernails and toenails.
5. Cervical lymphadenopathy
At least one enlarged lymph node may be present in the neck. It is usually unilateral and traditionally measures more than 1.5 cm.
Children may also experience marked irritability, joint pain, abdominal symptoms, vomiting, diarrhea, sterile pyuria, or mild hepatitis.
Incomplete Kawasaki Disease
Not every child develops all five classic clinical findings. Incomplete Kawasaki disease should be considered when a child has persistent unexplained fever with only two or three principal features, particularly when laboratory evidence of systemic inflammation is present.
Incomplete disease is especially important in infants younger than six months, who may present with prolonged fever and few other findings but remain at substantial risk of coronary complications. A lack of complete clinical criteria should not delay treatment when the overall presentation, laboratory testing, or echocardiogram supports the diagnosis.
Laboratory Findings
There is no single laboratory test that confirms Kawasaki disease. Testing instead supports the clinical diagnosis, evaluates the severity of inflammation, and helps exclude competing conditions.
Common findings include:
- Elevated C-reactive protein and erythrocyte sedimentation rate
- Neutrophilic leukocytosis during the acute phase
- Normocytic anemia
- Thrombocytosis, often developing after the first week
- Hypoalbuminemia
- Mild elevation of liver enzymes
- Sterile pyuria
- Hyponatremia in more severe disease
A complete blood count, comprehensive metabolic panel, inflammatory markers, albumin, liver testing, and urinalysis are frequently included in the initial evaluation. Cardiac biomarkers such as troponin or B-type natriuretic peptide may be obtained when myocarditis or ventricular dysfunction is suspected.
Echocardiography and Cardiac Testing
An echocardiogram should be performed when Kawasaki disease is diagnosed or strongly suspected. It evaluates:
- The size and appearance of the coronary arteries
- Left ventricular systolic function
- Pericardial effusion
- Valvular regurgitation
- Evidence of myocarditis
A normal initial echocardiogram does not exclude Kawasaki disease because coronary changes may develop later. Diagnosis and treatment should not be delayed solely because early imaging is normal.
Coronary artery dimensions are interpreted using Z scores, which compare the measured coronary diameter with the expected size for a child’s body surface area. Z scores help classify coronary involvement and determine the intensity of treatment, imaging, and long-term follow-up.
Conditions That Can Mimic Kawasaki Disease
The differential diagnosis includes:
- Viral infections, including adenovirus
- Scarlet fever
- Toxic shock syndrome
- Systemic juvenile idiopathic arthritis
- Drug hypersensitivity reactions
- Bacterial lymphadenitis
- Measles
- Multisystem inflammatory syndrome in children
Kawasaki Disease Versus MIS-C
MIS-C can produce fever, rash, conjunctival injection, oral changes, and cardiovascular involvement similar to Kawasaki disease. However, MIS-C generally occurs after SARS-CoV-2 infection and more commonly produces prominent gastrointestinal symptoms, shock, myocardial dysfunction, lymphopenia, and thrombocytopenia.
In contrast, classic Kawasaki disease more commonly affects younger children and is particularly associated with coronary artery inflammation and thrombocytosis during the later phase. Clinical overlap is substantial, so the distinction requires evaluation of the complete presentation, laboratory findings, cardiac imaging, and recent SARS-CoV-2 exposure or testing.
Initial Treatment
Children with suspected Kawasaki disease generally require hospital evaluation and treatment.
Intravenous Immunoglobulin
The standard initial treatment is intravenous immunoglobulin at 2 g/kg, administered as a single infusion. Treatment is ideally given within the first 10 days of illness and as soon as the diagnosis is established.
IVIG rapidly suppresses inflammation and significantly lowers the risk of coronary artery aneurysms.
Aspirin
Aspirin is administered during the acute inflammatory phase, although low-, moderate-, and high-dose protocols vary among institutions. Current evidence has not clearly shown that high-dose aspirin is superior to lower doses for preventing coronary complications.
After the fever and acute inflammation resolve, children are generally transitioned to low-dose aspirin for its antiplatelet effect. Aspirin may be discontinued after approximately four to six weeks when follow-up imaging shows normal coronary arteries and inflammatory markers have resolved. Children with persistent coronary abnormalities may need longer treatment.
Because aspirin use during influenza or varicella infection is associated with the risk of Reye syndrome, families should receive appropriate vaccination and illness-related counseling.
High-Risk Kawasaki Disease
Some children are at increased risk of IVIG resistance or coronary aneurysms. Relevant factors may include very young age, significant initial coronary enlargement, high inflammatory markers, shock, or severe cardiac involvement.
The 2024 American Heart Association update emphasizes early risk classification and more intensive initial treatment for high-risk patients. Selected children may receive corticosteroids or another anti-inflammatory agent in addition to IVIG.
IVIG-Resistant Kawasaki Disease
IVIG resistance is generally suspected when fever persists or returns after initial therapy. Management may include:
- A second IVIG infusion
- Corticosteroids
- Infliximab
- Other immunomodulatory treatment in selected refractory cases
Treatment should be coordinated with pediatric cardiology, rheumatology, infectious disease, or a specialized Kawasaki disease team.
Follow-Up After Treatment
Follow-up is based largely on coronary artery findings. Repeat echocardiography is generally performed during the illness and after discharge, with more frequent imaging when coronary dilation or aneurysms are present.
Monitoring may include:
- Fever and clinical symptoms
- CRP and ESR
- Platelet count
- Aspirin tolerance
- Coronary artery Z scores
- Ventricular function
- Evidence of thrombosis or arterial narrowing
Children without coronary involvement usually recover fully and may not require long-term specialist follow-up after the convalescent period. Patients with persistent moderate, large, or giant aneurysms need ongoing cardiology care, antithrombotic therapy, periodic cardiac imaging, and planned transition into adult cardiovascular care.
When to Seek Urgent Medical Evaluation
A child should receive prompt medical evaluation for an unexplained persistent fever accompanied by red eyes, rash, swollen hands or feet, cracked lips, strawberry tongue, or neck swelling.
Parents should not wait for every classic feature to appear. The findings may develop sequentially, disappear before evaluation, or remain incomplete—especially in young infants. Early recognition is central to preventing coronary complications.
Key Takeaway
Kawasaki disease is a clinical diagnosis that should be considered in children with persistent fever and mucocutaneous inflammation. There is no single confirmatory test, and a normal early echocardiogram does not rule it out.
Prompt treatment with IVIG and aspirin substantially lowers the risk of coronary artery aneurysms. High-risk or treatment-resistant cases may need additional anti-inflammatory therapy, while patients with coronary involvement require structured, long-term cardiac surveillance.
This article is intended for medical education and does not replace assessment or treatment by a pediatrician, pediatric cardiologist, or other qualified healthcare professional.