The ISCHEMIA trial was one of the most important cardiovascular trials evaluating whether an early invasive strategy improves outcomes in patients with stable coronary artery disease and moderate or severe ischemia.
For decades, many clinicians assumed that finding significant ischemia on stress testing meant that patients would benefit from early cardiac catheterization and revascularization. The ISCHEMIA trial challenged that assumption.
What Was the ISCHEMIA Trial?
The ISCHEMIA trial studied patients with stable coronary artery disease and moderate or severe ischemia on noninvasive stress testing.
Patients were randomized to one of two strategies:
- Initial invasive strategy
This included cardiac catheterization followed by revascularization when appropriate, in addition to guideline-directed medical therapy. - Initial conservative strategy
This involved guideline-directed medical therapy alone, with cardiac catheterization reserved for patients who failed medical therapy or developed worsening symptoms.
The goal of the ISCHEMIA trial was to determine whether an early invasive approach reduced major cardiovascular events compared with a conservative medical approach.
Study Design
The ISCHEMIA trial was a:
Multicenter, parallel, randomized controlled trial
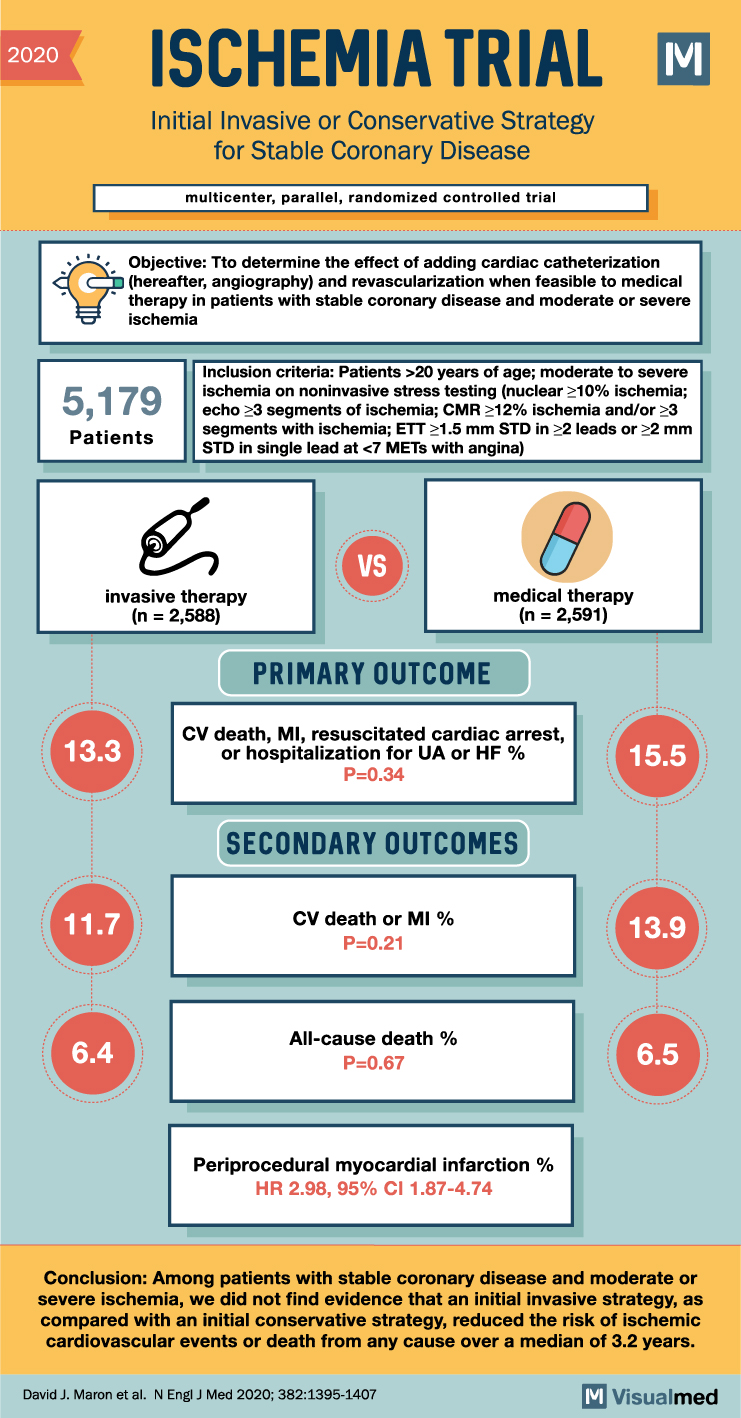
A total of 5,179 patients were enrolled.
Patients had stable coronary disease with evidence of moderate or severe ischemia. Importantly, this was not a trial of patients with acute coronary syndrome, unstable symptoms, or left main coronary disease requiring urgent intervention.
Who Was Included?
The ISCHEMIA trial included patients older than 20 years of age with moderate or severe ischemia on stress testing.
Examples of qualifying ischemia included:
- Nuclear stress testing showing at least 10% ischemia
- Echocardiography showing at least 3 ischemic segments
- Cardiac MRI showing at least 12% ischemic myocardium
- Exercise treadmill testing with significant ST depression and angina
The study population represented patients commonly seen in outpatient cardiology practice: stable symptoms, abnormal stress testing, and concern for obstructive coronary artery disease.
Treatment Groups
Patients were randomized into two groups:
Invasive therapy group
2,588 patients
These patients underwent cardiac catheterization with revascularization when appropriate, along with medical therapy.
Medical therapy group
2,591 patients
These patients were treated initially with guideline-directed medical therapy alone.
Primary Outcome
The primary outcome of the ISCHEMIA trial was a composite of:
- Cardiovascular death
- Myocardial infarction
- Resuscitated cardiac arrest
- Hospitalization for unstable angina
- Hospitalization for heart failure
The result:
- Invasive strategy: 13.3%
- Medical therapy: 15.5%
- P = 0.34
There was no statistically significant reduction in the primary outcome with an initial invasive strategy.
Secondary Outcomes
Cardiovascular death or myocardial infarction
- Invasive strategy: 11.7%
- Medical therapy: 13.9%
- P = 0.21
Again, there was no statistically significant difference.
All-cause death
- Invasive strategy: 6.4%
- Medical therapy: 6.5%
- P = 0.67
There was no mortality benefit with routine early invasive therapy.
Periprocedural myocardial infarction
The invasive strategy was associated with a higher risk of periprocedural myocardial infarction:
HR 2.98; 95% CI 1.87–4.74
This is an important tradeoff when considering early catheterization and revascularization in stable patients.
Main Finding of the ISCHEMIA Trial
The ISCHEMIA trial showed that in patients with stable coronary artery disease and moderate or severe ischemia, an initial invasive strategy did not significantly reduce major cardiovascular events or death compared with an initial conservative strategy over a median follow-up of 3.2 years.
In simple terms:
For stable coronary disease, abnormal stress testing alone does not automatically mean that early catheterization and revascularization improves survival or prevents heart attacks.
Clinical Meaning
The ISCHEMIA trial supports a more thoughtful approach to stable coronary disease.
For many stable patients, optimal medical therapy is a reasonable initial strategy. This includes:
- Antiplatelet therapy when appropriate
- High-intensity statin therapy
- Blood pressure control
- Antianginal medications
- Smoking cessation
- Diabetes management
- Lifestyle modification
However, this does not mean catheterization or revascularization is never useful.
Patients with persistent angina despite medical therapy may still benefit symptomatically from an invasive approach. The ISCHEMIA trial mainly tells us that routine early invasive management does not clearly reduce death or major ischemic events in stable patients.
Key Takeaway
The ISCHEMIA trial changed the way clinicians think about stable coronary artery disease.
For patients with stable symptoms and moderate or severe ischemia, starting with medical therapy is often safe and reasonable. An invasive strategy should be individualized, especially when symptoms remain significant despite optimal medical therapy.
Conclusion
The ISCHEMIA trial demonstrated that an initial invasive strategy did not significantly reduce cardiovascular events or death compared with an initial conservative strategy in patients with stable coronary disease and moderate or severe ischemia.