Severe acute malnutrition (SAM) remains one of the most difficult clinical settings in pediatric care, especially when complicated by gastroenteritis and dehydration. Clinicians are often cautious with intravenous fluids in these children because of concerns about fluid overload, electrolyte shifts, and clinical deterioration. Current WHO recommendations generally favor conservative rehydration strategies in children with SAM, but whether more active intravenous rehydration improves outcomes has remained uncertain.
The GASTROSAM trial was designed to answer an important practical question:
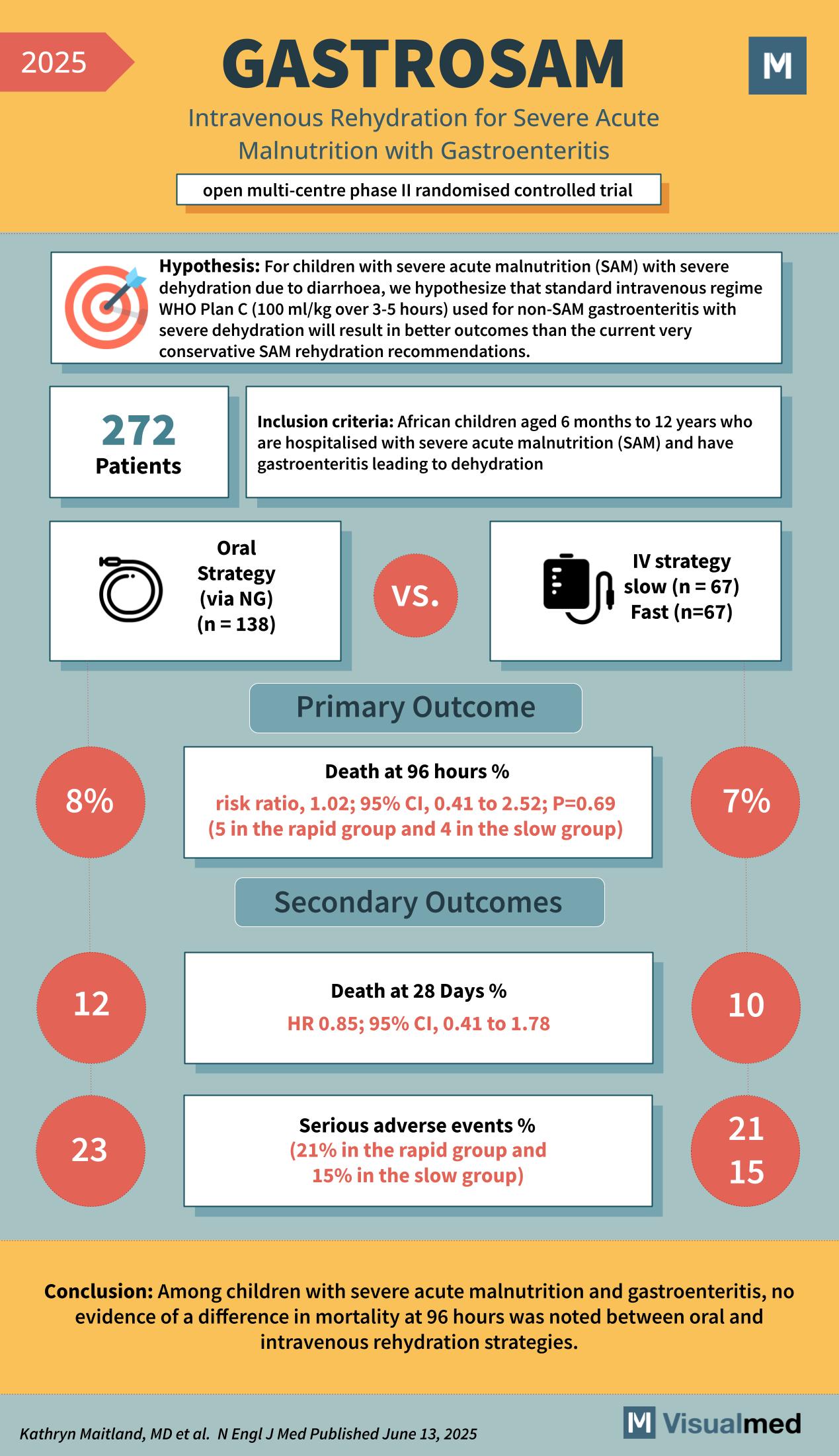
Does intravenous rehydration improve outcomes compared with oral or nasogastric rehydration in children with severe acute malnutrition and dehydration due to gastroenteritis?
Trial Design
GASTROSAM was an open-label, multicenter, phase 2 randomized controlled trial conducted in African children.
The study enrolled 272 children aged 6 months to 12 years who were hospitalized with:
- Severe acute malnutrition
- Gastroenteritis
- Clinical dehydration
Participants were assigned to either an oral rehydration strategy, usually via nasogastric tube when needed, or an intravenous rehydration strategy.
The treatment groups were:
- Oral strategy: 138 children
- IV strategy: 134 children
- Slow IV rehydration: 67 children
- Rapid IV rehydration: 67 children
The main hypothesis was that IV rehydration, using WHO Plan C-type fluid therapy, would lead to better outcomes than conservative SAM rehydration recommendations.
Primary Outcome
The primary outcome was death at 96 hours.
Mortality was very similar between the groups:
- Oral strategy: 8%
- IV strategy: 7%
The reported risk ratio was 1.02, with a 95% confidence interval of 0.41 to 2.52 and a P value of 0.69.
In practical terms, there was no evidence that intravenous rehydration reduced early mortality compared with oral or nasogastric rehydration.
Secondary Outcomes
At 28 days, mortality again did not clearly differ between groups:
- Oral strategy: 12%
- IV strategy: 10%
The hazard ratio was 0.85, with a 95% confidence interval of 0.41 to 1.78.
Serious adverse events were also reported:
- Oral strategy: 23%
- Rapid IV group: 21%
- Slow IV group: 15%
Although the slow IV group appeared numerically lower for serious adverse events, this phase 2 trial was not powered to establish a definitive safety advantage.
Clinical Interpretation
The key message from GASTROSAM is that intravenous rehydration did not show a mortality benefit over oral or nasogastric rehydration in children with severe acute malnutrition and gastroenteritis.
This is important because IV fluids are often viewed as a more aggressive and potentially more effective intervention in dehydrated children. However, in SAM, physiology is different. These children are vulnerable to fluid shifts, cardiac compromise, and metabolic instability. A more aggressive approach may not necessarily translate into better survival.
The trial supports the continued importance of careful, protocolized rehydration in children with SAM, with close monitoring rather than assuming IV therapy is superior.
Bottom Line
In the GASTROSAM randomized clinical trial, among children with severe acute malnutrition and gastroenteritis, there was no evidence of a difference in mortality at 96 hours between oral and intravenous rehydration strategies.
For clinicians, the takeaway is clear:
IV rehydration should not be assumed to improve outcomes in this high-risk population. Oral or nasogastric rehydration remains a reasonable and evidence-supported approach when clinically appropriate.