The FAME trial was a landmark cardiology trial that changed how interventional cardiologists think about coronary stenoses in patients with multivessel coronary artery disease. Instead of relying only on angiographic appearance, the FAME trial tested whether using fractional flow reserve, or FFR, to guide PCI could improve outcomes compared with angiography-guided PCI alone.
The main finding was that an FFR-guided PCI strategy reduced major adverse cardiovascular events at one year compared with angiography-guided PCI in patients with multivessel coronary artery disease.
Background: Why Was the FAME Trial Important?
In coronary angiography, a narrowing may look severe, but not every angiographic stenosis causes clinically significant ischemia. Before the FAME trial, many PCI decisions were based mainly on visual estimation of stenosis severity.
This created an important clinical question:
Should cardiologists stent every angiographically significant lesion, or should PCI be limited to lesions that are physiologically significant by FFR?
The FAME trial helped answer this by showing that physiology-guided revascularization can improve patient outcomes and reduce unnecessary stenting.
Study Design
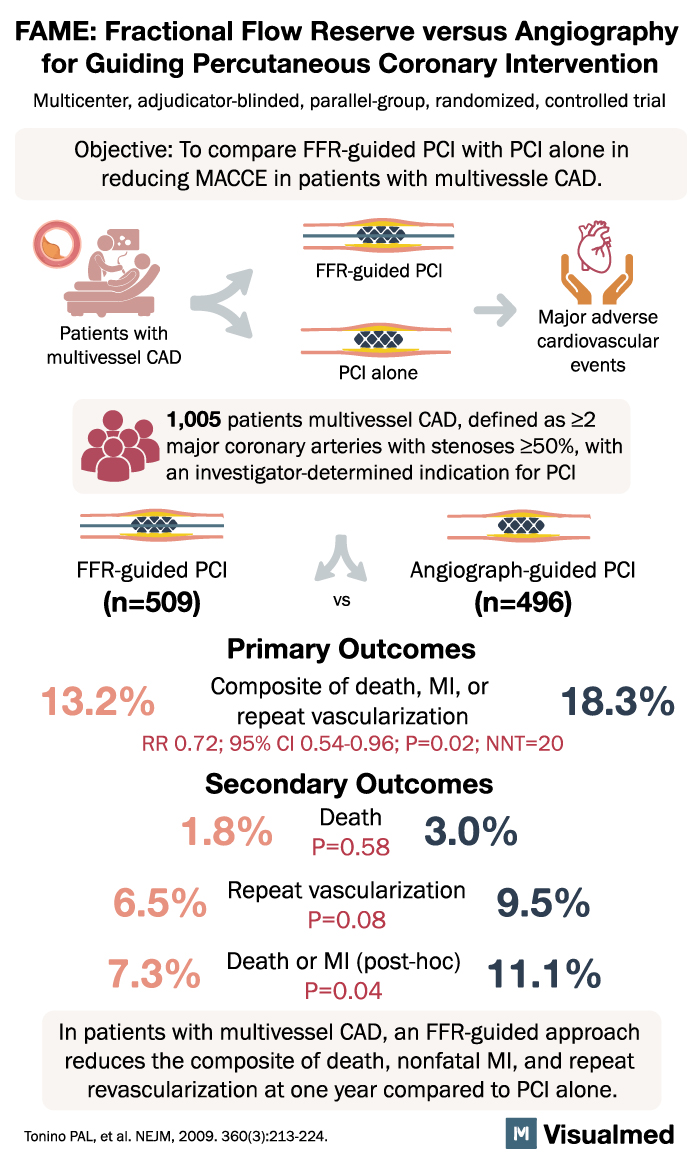
The FAME trial was a multicenter, adjudicator-blinded, parallel-group, randomized controlled trial.
It enrolled 1,005 patients with multivessel coronary artery disease. Multivessel CAD was defined as disease involving at least two major coronary arteries with stenosis of 50% or greater, where the treating investigator had determined that PCI was indicated.
Patients were randomized to:
- FFR-guided PCI
- Angiography-guided PCI
In the FFR-guided PCI group, only lesions with physiologic significance were treated. In the angiography-guided group, PCI decisions were made based on angiographic appearance alone.
Primary Outcome
The primary outcome of the FAME trial was a composite of:
Death, myocardial infarction, or repeat revascularization
At one year, the results were:
- FFR-guided PCI: 13.2%
- Angiography-guided PCI: 18.3%
This represented a significant reduction in major adverse cardiovascular events with FFR-guided PCI.
The relative risk was 0.72, with a 95% confidence interval of 0.54 to 0.96, and a P value of 0.02. The number needed to treat was approximately 20.
Secondary Outcomes
The FAME trial also evaluated important secondary outcomes.
Death
- FFR-guided PCI: 1.8%
- Angiography-guided PCI: 3.0%
This difference was not statistically significant.
Repeat Revascularization
- FFR-guided PCI: 6.5%
- Angiography-guided PCI: 9.5%
There was a numerical reduction in repeat revascularization with FFR-guided PCI.
Death or Myocardial Infarction
- FFR-guided PCI: 7.3%
- Angiography-guided PCI: 11.1%
This post-hoc endpoint favored the FFR-guided strategy.
Main Finding of the FAME Trial
The main message of the FAME trial was:
In patients with multivessel coronary artery disease, FFR-guided PCI reduced the composite outcome of death, myocardial infarction, or repeat revascularization at one year compared with angiography-guided PCI alone.
This showed that functional assessment of coronary lesions can be more clinically useful than relying only on how severe a blockage looks on angiography.
Clinical Interpretation
The FAME trial reinforced a major concept in coronary intervention:
Not every coronary stenosis that looks significant needs to be stented.
FFR allows cardiologists to determine whether a lesion is actually causing flow limitation and ischemia. By treating only physiologically significant lesions, patients may avoid unnecessary stents, procedural risks, and costs, while still receiving effective revascularization when it matters.
The trial supports:
- Physiology-guided PCI in multivessel CAD
- Avoiding PCI for non-ischemia-producing lesions
- More selective and evidence-based stent placement
- Better risk stratification during coronary angiography
- A shift from anatomy-only decision-making to physiology-guided care
Why the FAME Trial Still Matters
The FAME trial remains highly relevant because multivessel coronary artery disease is common, and angiographic severity alone can be misleading. A lesion that appears severe may not cause ischemia, while another lesion may be more clinically important than it looks.
FAME helped establish FFR as an important tool in the cath lab and influenced guideline recommendations for the assessment of intermediate coronary lesions.
The trial also set the stage for future studies evaluating physiology-guided revascularization strategies, including FAME 2 and other trials comparing invasive and conservative approaches in stable coronary disease.
Conclusion
The FAME trial showed that in patients with multivessel coronary artery disease, an FFR-guided PCI strategy reduced the composite of death, myocardial infarction, and repeat revascularization compared with angiography-guided PCI.
The practical takeaway is that PCI should not be guided by angiography alone when physiologic assessment is available. The FAME trial helped move interventional cardiology toward a more precise, patient-centered approach where lesions are treated based on ischemic significance rather than visual appearance alone.