The FAME 2 trial was a landmark cardiology trial that evaluated whether fractional flow reserve-guided PCI improves outcomes in patients with stable coronary artery disease and functionally significant coronary stenoses.
Unlike trials that relied mainly on angiographic stenosis, the FAME 2 trial selected patients based on fractional flow reserve, or FFR. Patients with an FFR of 0.80 or less were considered to have physiologically significant coronary lesions.
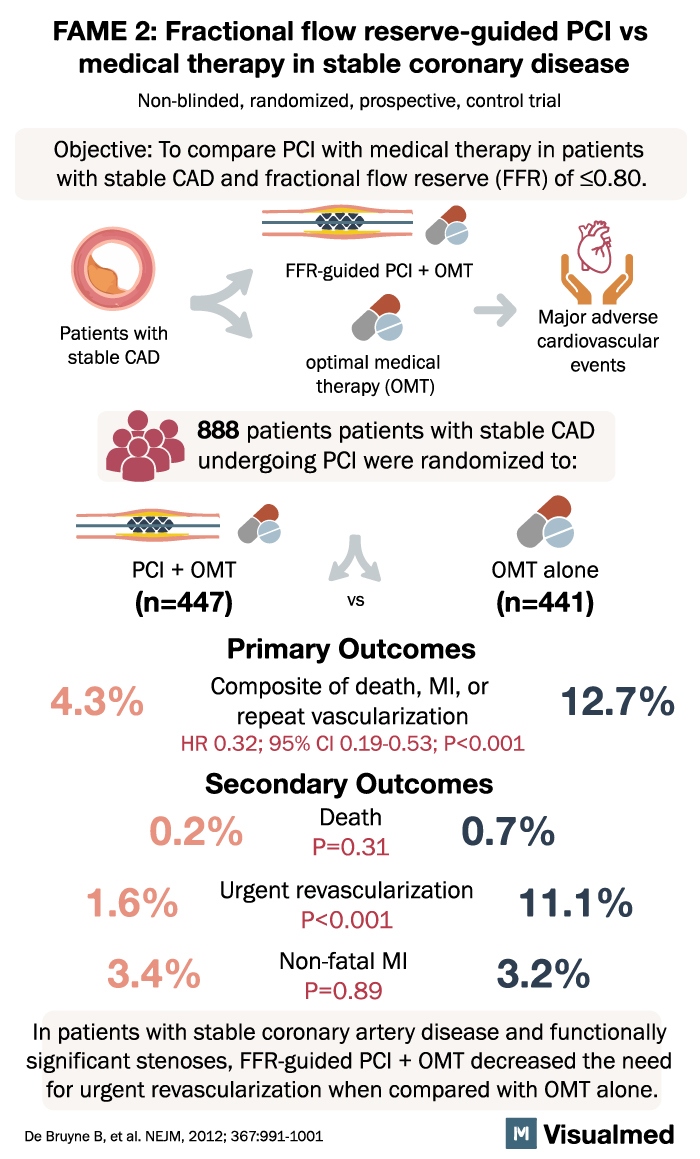
The main finding was that FFR-guided PCI plus optimal medical therapy reduced major adverse cardiovascular events compared with optimal medical therapy alone, mainly by lowering the need for urgent revascularization.
Background: Why Was the FAME 2 Trial Important?
Stable coronary artery disease is common, but not every coronary narrowing needs a stent. Angiography shows how a blockage looks, but it does not always show whether that blockage is actually limiting blood flow.
The FAME 2 trial was important because it focused on patients with functionally significant stenoses, meaning the lesions were not just visually narrowed but physiologically important by FFR.
The key clinical question was:
In patients with stable CAD and FFR-positive lesions, does PCI plus optimal medical therapy improve outcomes compared with optimal medical therapy alone?
Study Design
The FAME 2 trial was a non-blinded, randomized, prospective controlled trial.
It enrolled 888 patients with stable coronary artery disease and functionally significant stenoses based on FFR testing. Patients were randomized to:
- PCI plus optimal medical therapy
- Optimal medical therapy alone
The PCI group underwent FFR-guided revascularization in addition to guideline-directed medical therapy. The medical therapy group received optimal medical therapy without initial PCI.
Primary Outcome
The primary outcome of the FAME 2 trial was a composite of:
Death, myocardial infarction, or repeat revascularization
The results were:
- PCI plus optimal medical therapy: 4.3%
- Optimal medical therapy alone: 12.7%
This was a statistically significant reduction in the primary composite outcome with PCI plus medical therapy.
The hazard ratio was 0.32, with a 95% confidence interval of 0.19 to 0.53, and a P value of <0.001.
Secondary Outcomes
The FAME 2 trial also evaluated individual clinical outcomes.
Death
- PCI plus optimal medical therapy: 0.2%
- Optimal medical therapy alone: 0.7%
This difference was not statistically significant.
Urgent Revascularization
- PCI plus optimal medical therapy: 1.6%
- Optimal medical therapy alone: 11.1%
This was the major driver of benefit in the trial and strongly favored the PCI plus medical therapy group.
Nonfatal Myocardial Infarction
- PCI plus optimal medical therapy: 3.4%
- Optimal medical therapy alone: 3.2%
There was no significant difference in nonfatal myocardial infarction between the groups.
Main Finding of the FAME 2 Trial
The main message of the FAME 2 trial was:
In patients with stable coronary artery disease and FFR-positive coronary stenoses, FFR-guided PCI plus optimal medical therapy reduced major adverse cardiovascular events compared with optimal medical therapy alone, primarily by reducing urgent revascularization.
This is an important distinction. The trial did not show a major reduction in death or nonfatal myocardial infarction. The benefit was mainly driven by fewer urgent revascularization procedures.
Clinical Interpretation
The FAME 2 trial supports the idea that physiology matters. In stable coronary artery disease, PCI is more likely to be beneficial when the lesion is proven to be functionally significant.
This trial helped strengthen the role of FFR in decision-making for stable CAD. Rather than stenting lesions based only on angiographic appearance, clinicians can use FFR to identify which stenoses are actually causing ischemia.
The practical implications are:
- FFR can help identify patients most likely to benefit from PCI
- FFR-guided PCI can reduce urgent revascularization
- PCI should be targeted to physiologically significant lesions
- Medical therapy remains essential in both treatment strategies
- The main benefit of PCI in this trial was not mortality reduction, but reduction in urgent revascularization
FAME 2 Trial Compared With FAME Trial
The original FAME trial compared FFR-guided PCI with angiography-guided PCI in patients with multivessel coronary artery disease. It showed that FFR-guided PCI improved outcomes compared with angiography-guided PCI.
The FAME 2 trial asked a different question. It compared FFR-guided PCI plus optimal medical therapy against optimal medical therapy alone in stable CAD patients with FFR-positive lesions.
Together, FAME and FAME 2 helped establish that coronary physiology should guide PCI decisions, especially in stable coronary disease.
Why the FAME 2 Trial Still Matters
The FAME 2 trial remains clinically relevant because it helps define when PCI may be useful in stable CAD. It does not support routine PCI for every angiographic narrowing. Instead, it supports a more selective approach where PCI is considered when a lesion is physiologically significant.
In daily practice, this means FFR can help avoid unnecessary stenting while identifying patients who may benefit from revascularization.
Conclusion
The FAME 2 trial showed that in patients with stable coronary artery disease and FFR-positive stenoses, FFR-guided PCI plus optimal medical therapy reduced major adverse cardiovascular events compared with optimal medical therapy alone.
The benefit was mainly due to a reduction in urgent revascularization, with no significant reduction in death or nonfatal myocardial infarction. The trial reinforced the importance of physiology-guided decision-making in stable coronary artery disease.