The CURE trial was a landmark randomized clinical trial that evaluated whether adding clopidogrel to aspirin improves outcomes in patients with non–ST-elevation acute coronary syndrome, including NSTEMI and unstable angina.
The main finding was: clopidogrel plus aspirin reduced cardiovascular death, nonfatal MI, or stroke, but increased major bleeding.
Background
Patients with NSTEMI or unstable angina are at high risk for recurrent ischemic events after presentation. Aspirin was already standard therapy, but aspirin alone does not fully suppress platelet activation.
The CURE trial tested whether adding a second antiplatelet agent, clopidogrel, to aspirin would reduce future cardiovascular events in this high-risk population.
This trial became one of the key studies supporting dual antiplatelet therapy in acute coronary syndrome.
Objective of the CURE Trial
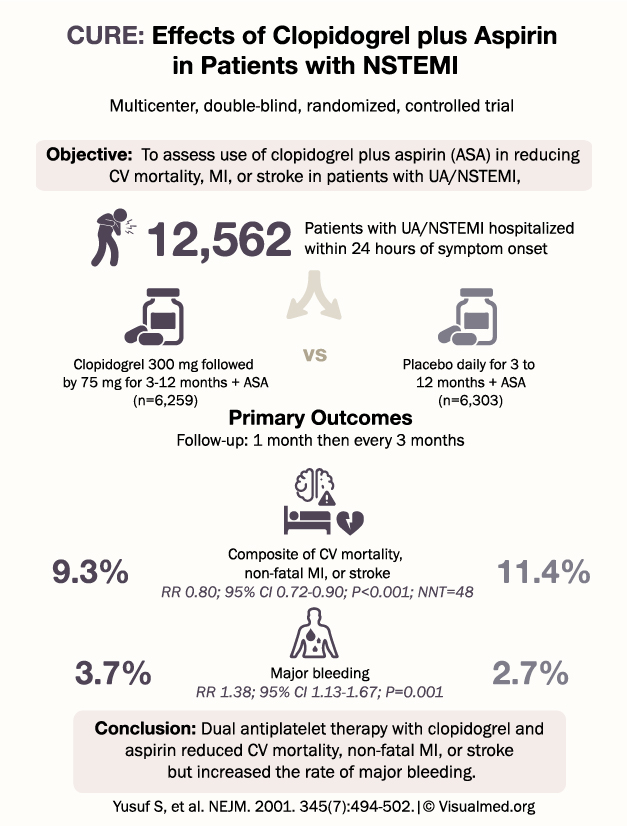
The objective was to assess whether clopidogrel plus aspirin reduces:
Cardiovascular death, myocardial infarction, or stroke
in patients hospitalized with unstable angina or NSTEMI.
Study Design
The CURE trial was a:
Multicenter, double-blind, randomized, controlled trial
A total of 12,562 patients were enrolled.
Patients had UA/NSTEMI and were hospitalized within 24 hours of symptom onset.
They were randomized to:
- Clopidogrel plus aspirin
Clopidogrel 300 mg loading dose, followed by 75 mg daily for 3 to 12 months
n = 6,259 - Placebo plus aspirin
Placebo daily for 3 to 12 months
n = 6,303
Follow-up occurred at 1 month and then every 3 months.
Primary Outcome
The primary outcome was the composite of:
Cardiovascular mortality, nonfatal myocardial infarction, or stroke
Results:
Clopidogrel + aspirin: 9.3%
Placebo + aspirin: 11.4%
Risk reduction:
RR 0.80; 95% CI, 0.72 to 0.90; P < 0.001
Number needed to treat:
NNT 48
This showed that adding clopidogrel to aspirin significantly reduced major cardiovascular events in patients with UA/NSTEMI.
Bleeding Risk
Major bleeding occurred in:
Clopidogrel + aspirin: 3.7%
Placebo + aspirin: 2.7%
Risk increase:
RR 1.38; 95% CI, 1.13 to 1.67; P = 0.001
So the benefit came with a clear tradeoff: fewer ischemic events, but more major bleeding.
Why the CURE Trial Matters
The CURE trial helped establish the foundation for dual antiplatelet therapy in patients with non-ST-elevation ACS.
Before this trial, aspirin was a mainstay of therapy, but the role of adding clopidogrel early and continuing it after hospitalization was less clearly defined.
CURE showed that dual antiplatelet therapy could meaningfully reduce ischemic events in UA/NSTEMI patients, even though bleeding risk increased.
Clinical Takeaway
The main takeaway from the CURE trial is:
In patients with unstable angina or NSTEMI, clopidogrel added to aspirin reduced cardiovascular death, nonfatal MI, or stroke compared with aspirin alone, but increased major bleeding.
This trial supports the principle that patients with ACS benefit from more intensive platelet inhibition, provided bleeding risk is acceptable.
Practical Interpretation
Clopidogrel plus aspirin may be beneficial in NSTEMI/unstable angina patients who have:
- High ischemic risk
- Troponin-positive ACS
- Recurrent angina
- Planned invasive or conservative management
- Acceptable bleeding risk
Greater caution is needed in patients with:
- High bleeding risk
- Active bleeding
- Severe anemia
- Need for urgent surgery
- Need for anticoagulation
- Frailty or prior major bleeding
Conclusion
The CURE trial demonstrated that adding clopidogrel to aspirin in patients with NSTEMI or unstable angina significantly reduced cardiovascular death, nonfatal myocardial infarction, or stroke.
However, this came at the cost of increased major bleeding.
In simple terms: CURE established that dual antiplatelet therapy with clopidogrel and aspirin improves ischemic outcomes in NSTEMI/unstable angina, but bleeding risk must be carefully considered.