The TRITON-TIMI 38 trial was a major randomized clinical trial comparing prasugrel with clopidogrel in patients with acute coronary syndrome who were scheduled to undergo PCI.
The main finding was: prasugrel reduced ischemic cardiovascular events compared with clopidogrel, but increased bleeding risk.
Background
Patients with acute coronary syndrome are at high risk for recurrent cardiovascular events, especially after PCI. Antiplatelet therapy is central to preventing stent thrombosis, recurrent myocardial infarction, and cardiovascular death.
For many years, clopidogrel was the standard P2Y12 inhibitor used with aspirin. The TRITON-TIMI 38 trial tested whether prasugrel, a more potent antiplatelet agent, would improve outcomes compared with clopidogrel in ACS patients undergoing PCI.
Objective of the TRITON-TIMI 38 Trial
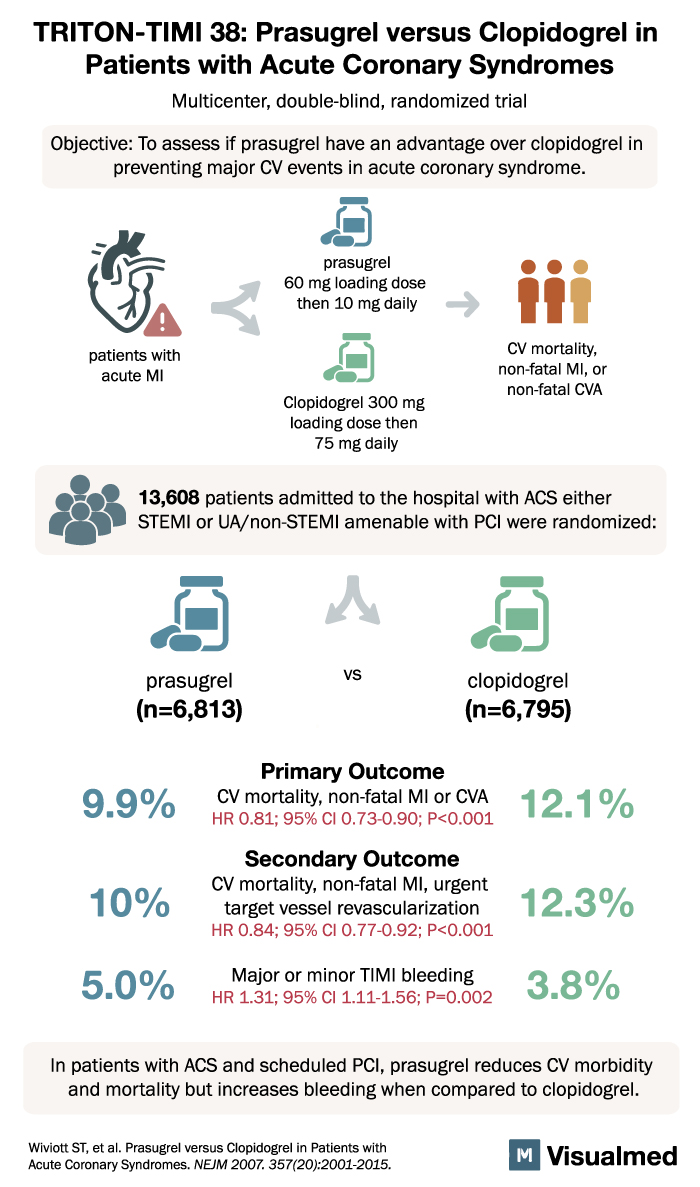
The objective was to determine whether prasugrel had an advantage over clopidogrel in preventing major cardiovascular events in patients with acute coronary syndrome.
The main clinical outcome was:
Cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke
Study Design
TRITON-TIMI 38 was a:
Multicenter, double-blind, randomized trial
A total of 13,608 patients were enrolled.
Patients were admitted with acute coronary syndrome, including:
- STEMI
- Unstable angina/non-STEMI
All patients were scheduled for PCI.
Patients were randomized to:
- Prasugrel
60 mg loading dose, then 10 mg daily
n = 6,813 - Clopidogrel
300 mg loading dose, then 75 mg daily
n = 6,795
Primary Outcome
The primary outcome was:
Cardiovascular mortality, nonfatal myocardial infarction, or nonfatal stroke
Results:
Prasugrel: 9.9%
Clopidogrel: 12.1%
Risk reduction:
HR 0.81; 95% CI, 0.73 to 0.90; P < 0.001
This showed that prasugrel significantly reduced major ischemic cardiovascular events compared with clopidogrel.
Secondary Outcome
A key secondary outcome was:
Cardiovascular mortality, nonfatal myocardial infarction, or urgent target vessel revascularization
Results:
Prasugrel: 10.0%
Clopidogrel: 12.3%
Risk reduction:
HR 0.84; 95% CI, 0.77 to 0.92; P < 0.001
This reinforced the ischemic benefit of prasugrel in ACS patients undergoing PCI.
Bleeding Outcome
The major safety issue was bleeding.
Major or minor TIMI bleeding occurred in:
Prasugrel: 5.0%
Clopidogrel: 3.8%
Risk increase:
HR 1.31; 95% CI, 1.11 to 1.56; P = 0.002
So while prasugrel reduced ischemic events, it also increased bleeding complications.
Why TRITON-TIMI 38 Matters
The TRITON-TIMI 38 trial helped establish prasugrel as a more potent alternative to clopidogrel in selected ACS patients undergoing PCI.
The trial showed a classic tradeoff:
More ischemic protection, more bleeding.
This matters because antiplatelet therapy is not just about preventing MI or stent thrombosis. It is about balancing the benefit of stronger platelet inhibition against the harm of bleeding.
Clinical Takeaway
The main takeaway from TRITON-TIMI 38 is:
In ACS patients scheduled for PCI, prasugrel reduced cardiovascular death, nonfatal MI, or nonfatal stroke compared with clopidogrel, but increased major or minor TIMI bleeding.
This means prasugrel can be a strong option when ischemic risk is high and bleeding risk is acceptable.
Practical Interpretation
Prasugrel may be favored in ACS patients undergoing PCI who have:
- High ischemic risk
- Diabetes
- Large thrombus burden
- STEMI presentation
- Low bleeding risk
- No contraindications to prasugrel
Clopidogrel may be preferred when bleeding risk is high or when prasugrel is not appropriate.
In real-world practice, prasugrel is generally avoided in patients with prior stroke or TIA, and caution is used in older or lower-body-weight patients because of bleeding concerns.
Conclusion
The TRITON-TIMI 38 trial demonstrated that prasugrel was superior to clopidogrel in reducing ischemic cardiovascular outcomes among patients with acute coronary syndrome undergoing PCI.
However, this benefit came with a significant increase in bleeding.
In simple terms: prasugrel is stronger than clopidogrel for preventing ischemic events after ACS PCI, but the price is more bleeding — so patient selection is critical.