The PLATO trial was a landmark cardiovascular trial comparing ticagrelor with clopidogrel in patients presenting with acute coronary syndrome.
The main finding was clear: ticagrelor reduced cardiovascular death, myocardial infarction, or stroke compared with clopidogrel, without a significant increase in major bleeding.
Background
Patients with acute coronary syndrome, including STEMI and non-STEMI, are at high risk for recurrent ischemic events after presentation. Platelet activation plays a central role in coronary thrombosis, so antiplatelet therapy is a cornerstone of ACS treatment.
For years, clopidogrel was widely used as the standard P2Y12 inhibitor. The PLATO trial tested whether ticagrelor, a more potent and reversible P2Y12 inhibitor, could improve outcomes compared with clopidogrel.
Objective of the PLATO Trial
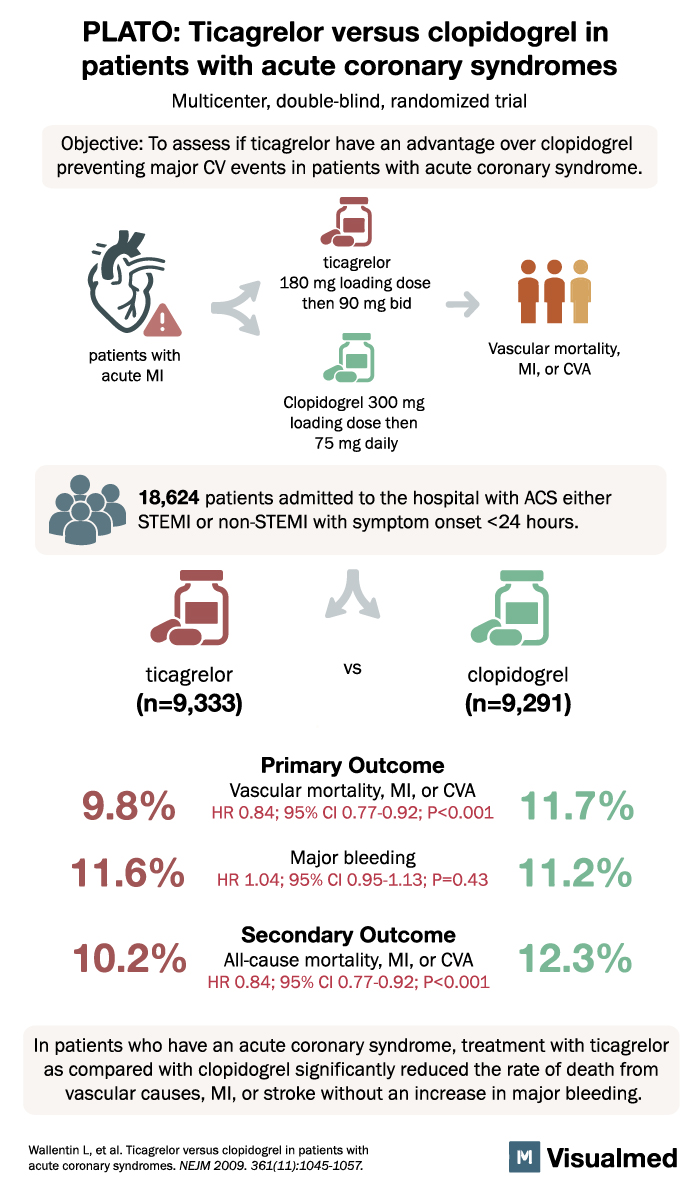
The objective of the PLATO trial was to determine whether ticagrelor was superior to clopidogrel in preventing major cardiovascular events in patients with acute coronary syndrome.
The key outcome of interest was:
Vascular death, myocardial infarction, or stroke
Study Design
The PLATO trial was a:
Multicenter, double-blind, randomized trial
A total of 18,624 patients were enrolled.
Patients were admitted to the hospital with acute coronary syndrome, including either:
- STEMI
- Non-STEMI
Symptom onset was within 24 hours.
Patients were randomized to one of two treatment groups:
- Ticagrelor
180 mg loading dose, then 90 mg twice daily
n = 9,333 - Clopidogrel
300 mg loading dose, then 75 mg daily
n = 9,291
Primary Outcome
The primary outcome was:
Vascular mortality, myocardial infarction, or stroke
Results:
Ticagrelor: 9.8%
Clopidogrel: 11.7%
Risk reduction:
HR 0.84; 95% CI, 0.77 to 0.92; P < 0.001
This showed that ticagrelor significantly reduced the risk of major cardiovascular events compared with clopidogrel.
Major Bleeding
Major bleeding occurred in:
Ticagrelor: 11.6%
Clopidogrel: 11.2%
Risk comparison:
HR 1.04; 95% CI, 0.95 to 1.13; P = 0.43
There was no statistically significant increase in major bleeding with ticagrelor compared with clopidogrel.
This is a key reason the trial was so influential: ticagrelor improved ischemic outcomes without significantly increasing overall major bleeding.
Secondary Outcome
The secondary outcome was:
All-cause mortality, myocardial infarction, or stroke
Results:
Ticagrelor: 10.2%
Clopidogrel: 12.3%
Risk reduction:
HR 0.84; 95% CI, 0.77 to 0.92; P < 0.001
This confirmed that ticagrelor provided broader clinical benefit beyond the primary endpoint.
Why the PLATO Trial Matters
The PLATO trial changed the treatment landscape for acute coronary syndrome.
Before PLATO, clopidogrel was a dominant antiplatelet therapy for ACS. PLATO showed that ticagrelor was more effective at preventing major ischemic events.
The trial helped establish ticagrelor as an important treatment option for ACS patients, especially those at higher ischemic risk.
Clinical Takeaway
The main takeaway from the PLATO trial is:
In patients with acute coronary syndrome, ticagrelor reduced vascular death, myocardial infarction, or stroke compared with clopidogrel, without a significant increase in major bleeding.
This makes ticagrelor a stronger antiplatelet option than clopidogrel for many ACS patients.
Practical Interpretation
Ticagrelor may be preferred over clopidogrel in ACS patients when bleeding risk is acceptable and there are no major contraindications.
However, clopidogrel may still be reasonable in certain patients, such as those with:
- High bleeding risk
- Need for oral anticoagulation
- Cost or access barriers
- Poor tolerance of ticagrelor
- Significant dyspnea with ticagrelor
- Bradyarrhythmia concerns
So the PLATO trial supports ticagrelor as a superior ischemic-risk reduction strategy, but real-world patient selection still matters.
Conclusion
The PLATO trial demonstrated that in patients hospitalized with acute coronary syndrome, ticagrelor was superior to clopidogrel in reducing vascular death, myocardial infarction, or stroke.
Importantly, this benefit occurred without a significant increase in major bleeding.
In simple terms: for ACS patients, ticagrelor beat clopidogrel for preventing major cardiovascular events, while overall major bleeding remained similar.