The DAPT trial was a major randomized clinical trial that evaluated whether extending dual antiplatelet therapy beyond 12 months after drug-eluting stent placement improves cardiovascular outcomes.
The trial showed that continued dual antiplatelet therapy reduced stent thrombosis and major adverse cardiovascular and cerebrovascular events, but this benefit came at the cost of increased bleeding.
Background
After PCI with a drug-eluting stent, patients are typically treated with dual antiplatelet therapy, usually aspirin plus a P2Y12 inhibitor such as clopidogrel or prasugrel.
The purpose of DAPT is to reduce the risk of stent thrombosis and ischemic events after coronary stenting.
The key clinical question was:
Should patients continue DAPT beyond 12 months after drug-eluting stent implantation, or should they stop the P2Y12 inhibitor and continue aspirin alone?
The DAPT trial was designed to answer this question.
Objective of the DAPT Trial
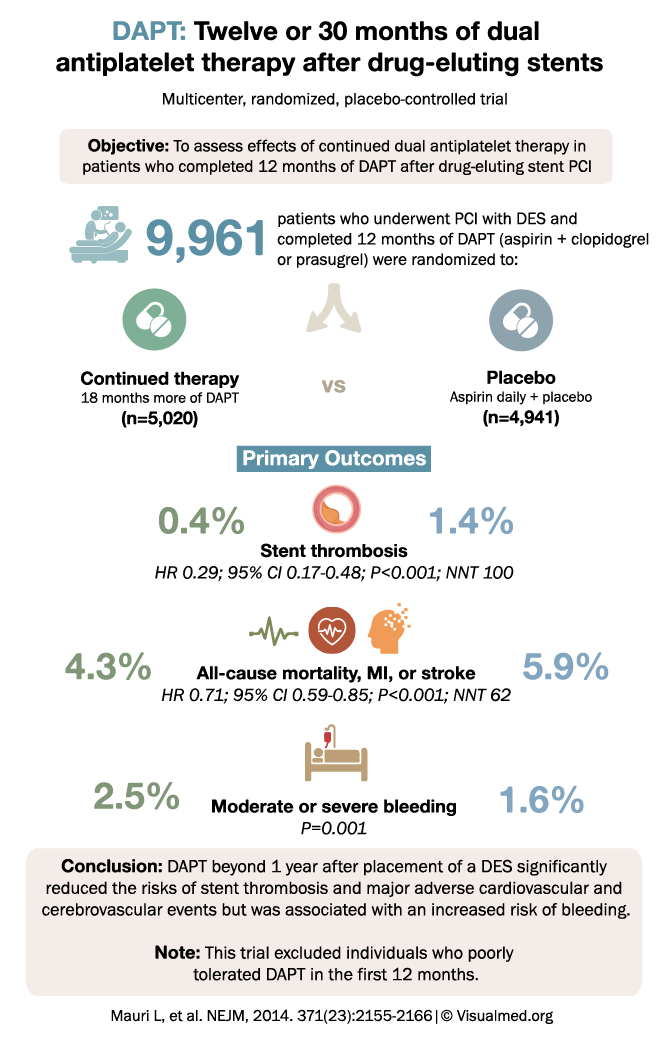
The objective was to assess the effects of continued dual antiplatelet therapy in patients who had already completed 12 months of DAPT after drug-eluting stent PCI.
Study Design
The DAPT trial was a:
Multicenter, randomized, placebo-controlled trial
A total of 9,961 patients were included.
All patients had undergone PCI with a drug-eluting stent and had completed 12 months of DAPT with:
Aspirin plus clopidogrel or prasugrel
After completing 12 months of DAPT, patients were randomized to:
- Continued therapy
18 additional months of DAPT
n = 5,020 - Placebo
Aspirin daily plus placebo
n = 4,941
Primary Outcomes
Stent Thrombosis
Stent thrombosis occurred in:
Continued DAPT: 0.4%
Placebo: 1.4%
This was a significant reduction:
HR 0.29; 95% CI, 0.17 to 0.48; P < 0.001
The number needed to treat was:
NNT 100
This means that extended DAPT substantially reduced the risk of stent thrombosis after drug-eluting stent placement.
Major Cardiovascular and Cerebrovascular Events
The composite outcome of:
All-cause mortality, myocardial infarction, or stroke
occurred in:
Continued DAPT: 4.3%
Placebo: 5.9%
Risk reduction:
HR 0.71; 95% CI, 0.59 to 0.85; P < 0.001
The number needed to treat was:
NNT 62
This showed that continuing DAPT beyond 12 months lowered the risk of major ischemic events.
Bleeding Risk
Moderate or severe bleeding occurred in:
Continued DAPT: 2.5%
Placebo: 1.6%
This was statistically significant:
P = 0.001
So while extended DAPT reduced ischemic events, it also increased bleeding risk.
Why the DAPT Trial Matters
The DAPT trial helped define the tradeoff between ischemic protection and bleeding risk after drug-eluting stent PCI.
Longer DAPT was not simply “better” for everyone. It reduced stent thrombosis and major ischemic events, but at the cost of more bleeding.
This made individualized decision-making essential.
Patients at high ischemic risk and low bleeding risk may benefit from longer DAPT. Patients at high bleeding risk may be better served by shorter therapy.
Important Trial Note
A key limitation is that the trial included patients who had already tolerated the first 12 months of DAPT.
This matters because patients who had major bleeding, intolerance, or early complications during the first year were not the same population being tested.
So the results apply best to patients who:
Successfully completed 12 months of DAPT without major problems.
Clinical Takeaway
The main takeaway from the DAPT trial is:
Extending dual antiplatelet therapy beyond 1 year after drug-eluting stent placement reduces stent thrombosis and major cardiovascular/cerebrovascular events, but increases moderate or severe bleeding.
In practice, the decision to extend DAPT should depend on the patient’s balance of:
Ischemic risk
versus
Bleeding risk
Practical Interpretation
Extended DAPT may be reasonable in patients with:
- Prior myocardial infarction
- Complex PCI
- Multiple stents
- Diabetes
- High ischemic risk
- Low bleeding risk
- Good tolerance of DAPT during the first year
Shorter DAPT or stopping the P2Y12 inhibitor after 12 months may be preferred in patients with:
- Prior bleeding
- High bleeding risk
- Need for anticoagulation
- Frailty
- Anemia
- Poor tolerance of antiplatelet therapy
Conclusion
The DAPT trial demonstrated that continuing dual antiplatelet therapy for 30 months after drug-eluting stent placement reduced stent thrombosis and major adverse cardiovascular and cerebrovascular events compared with stopping DAPT after 12 months.
However, this benefit came with an increased risk of bleeding.
In simple terms: longer DAPT protects against ischemic events, but increases bleeding — so patient selection is everything.