The CULPRIT-SHOCK trial was an important randomized clinical trial that changed how interventional cardiologists think about PCI strategy in patients with acute myocardial infarction complicated by cardiogenic shock.
The main finding was clinically important: in patients with AMI and cardiogenic shock, culprit-lesion-only PCI had better early outcomes than immediate multivessel PCI.
Background
Patients with acute myocardial infarction sometimes present with cardiogenic shock, a life-threatening condition where the heart cannot pump enough blood to maintain adequate organ perfusion.
Many of these patients also have multivessel coronary artery disease, meaning there are significant blockages in more than one coronary artery.
The key question was:
Should doctors open only the artery causing the heart attack, or should they immediately treat multiple blocked arteries during the same procedure?
The CULPRIT-SHOCK trial tested these two strategies.
Objective of the CULPRIT-SHOCK Trial
The objective of the trial was to compare clinical outcomes after:
Culprit-lesion-only PCI
versus
Immediate multivessel PCI
in patients with acute myocardial infarction and cardiogenic shock.
Study Design
The CULPRIT-SHOCK trial was a:
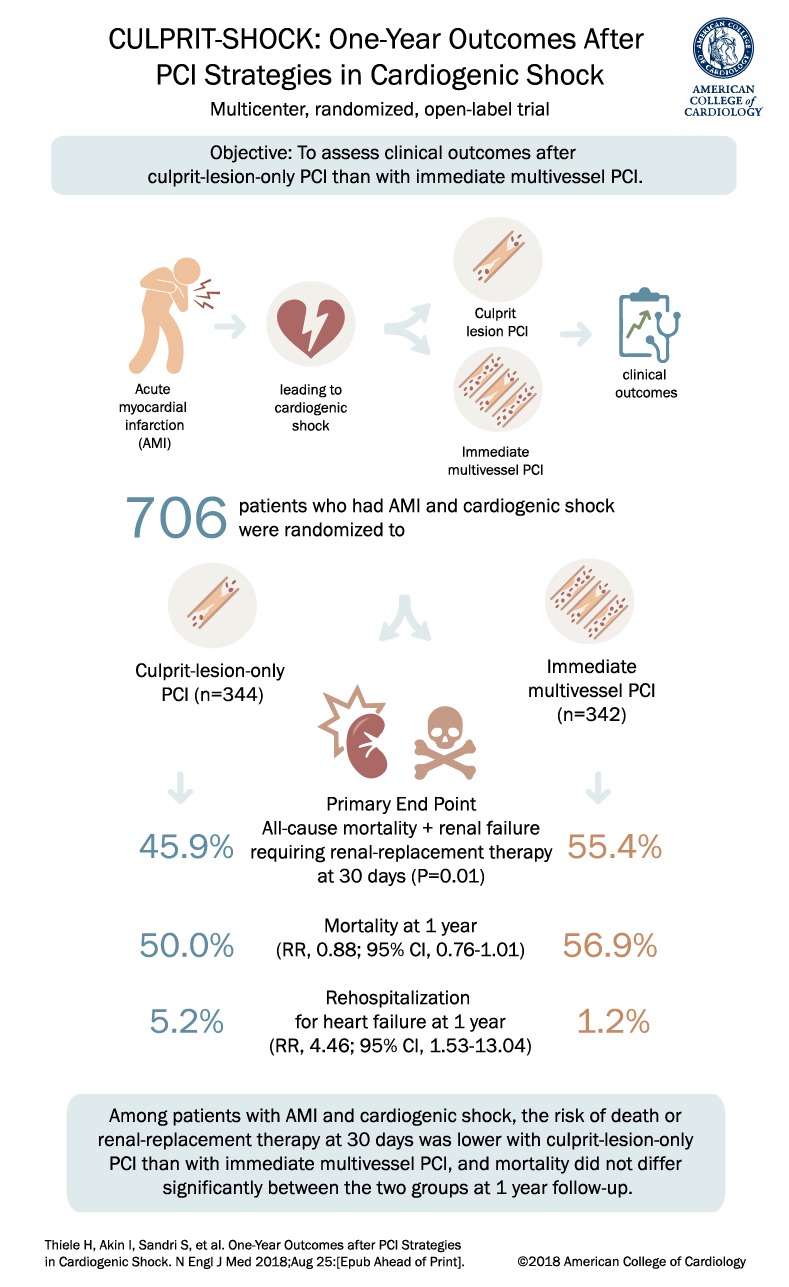
Multicenter, randomized, open-label trial
A total of 706 patients with acute myocardial infarction and cardiogenic shock were randomized.
Patients were assigned to one of two PCI strategies:
- Culprit-lesion-only PCI
n = 344 - Immediate multivessel PCI
n = 342
Primary End Point
The primary end point was:
All-cause mortality or renal failure requiring renal-replacement therapy at 30 days
Results:
Culprit-lesion-only PCI: 45.9%
Immediate multivessel PCI: 55.4%
The result favored culprit-lesion-only PCI:
P = 0.01
This means that treating only the culprit lesion initially reduced the combined risk of death or severe kidney failure requiring dialysis at 30 days compared with immediately treating multiple vessels.
One-Year Mortality
At 1 year, mortality was:
Culprit-lesion-only PCI: 50.0%
Immediate multivessel PCI: 56.9%
Relative risk:
RR 0.88; 95% CI, 0.76 to 1.01
Mortality at 1 year was numerically lower with culprit-lesion-only PCI, but it was not statistically significantly different between the two groups.
Rehospitalization for Heart Failure
Rehospitalization for heart failure at 1 year was:
Culprit-lesion-only PCI: 5.2%
Immediate multivessel PCI: 1.2%
Relative risk:
RR 4.46; 95% CI, 1.53 to 13.04
This outcome was higher in the culprit-lesion-only PCI group, which is an important nuance. While culprit-lesion-only PCI improved the early primary outcome, there was a higher rate of rehospitalization for heart failure at 1 year.
Why the CULPRIT-SHOCK Trial Matters
The CULPRIT-SHOCK trial is important because it challenged the assumption that “more complete” PCI during the initial procedure is always better.
In stable STEMI patients with multivessel disease, complete revascularization can improve outcomes, as shown in trials such as COMPLETE. But cardiogenic shock is different.
These patients are critically ill. Longer procedures, more contrast exposure, and additional vessel manipulation may increase risk during the acute phase.
The CULPRIT-SHOCK trial suggested that in the setting of cardiogenic shock, the safer initial approach is usually to stabilize the patient by treating the culprit artery first, rather than performing immediate multivessel PCI.
Clinical Takeaway
The main takeaway from the CULPRIT-SHOCK trial is:
In patients with acute myocardial infarction and cardiogenic shock, culprit-lesion-only PCI reduced the risk of death or renal-replacement therapy at 30 days compared with immediate multivessel PCI.
At 1 year, mortality was not significantly different between the two strategies.
Practical Interpretation
For a patient with AMI and cardiogenic shock:
Initial strategy: Treat the culprit lesion first.
Avoid: Routine immediate multivessel PCI during the shock presentation.
Consider later: Staged revascularization of nonculprit lesions once the patient is stabilized, depending on anatomy, ischemia, symptoms, and clinical status.
Conclusion
The CULPRIT-SHOCK trial showed that among patients with acute myocardial infarction and cardiogenic shock, culprit-lesion-only PCI was superior to immediate multivessel PCI for reducing the 30-day composite outcome of death or renal failure requiring renal-replacement therapy.
This trial supports a more conservative initial PCI strategy in cardiogenic shock: open the culprit artery, stabilize the patient, and consider additional revascularization later when appropriate.