The COMPLETE trial was a landmark randomized clinical trial that evaluated whether patients with ST-segment elevation myocardial infarction (STEMI) and multivessel coronary artery disease benefit from complete revascularization rather than treating only the culprit lesion.
The key finding was clear: complete revascularization with multivessel PCI reduced major cardiovascular events compared with culprit-lesion-only PCI.
Background
In patients presenting with STEMI, the immediate priority is opening the culprit coronary artery responsible for the acute myocardial infarction. However, many patients also have significant disease in other coronary arteries.
The clinical question has always been: should those nonculprit lesions be treated as well?
Historically, many operators focused only on the culprit lesion during the acute event, leaving other stenoses for medical therapy or later consideration. The COMPLETE trial tested whether a strategy of planned complete revascularization would improve outcomes.
Objective of the COMPLETE Trial
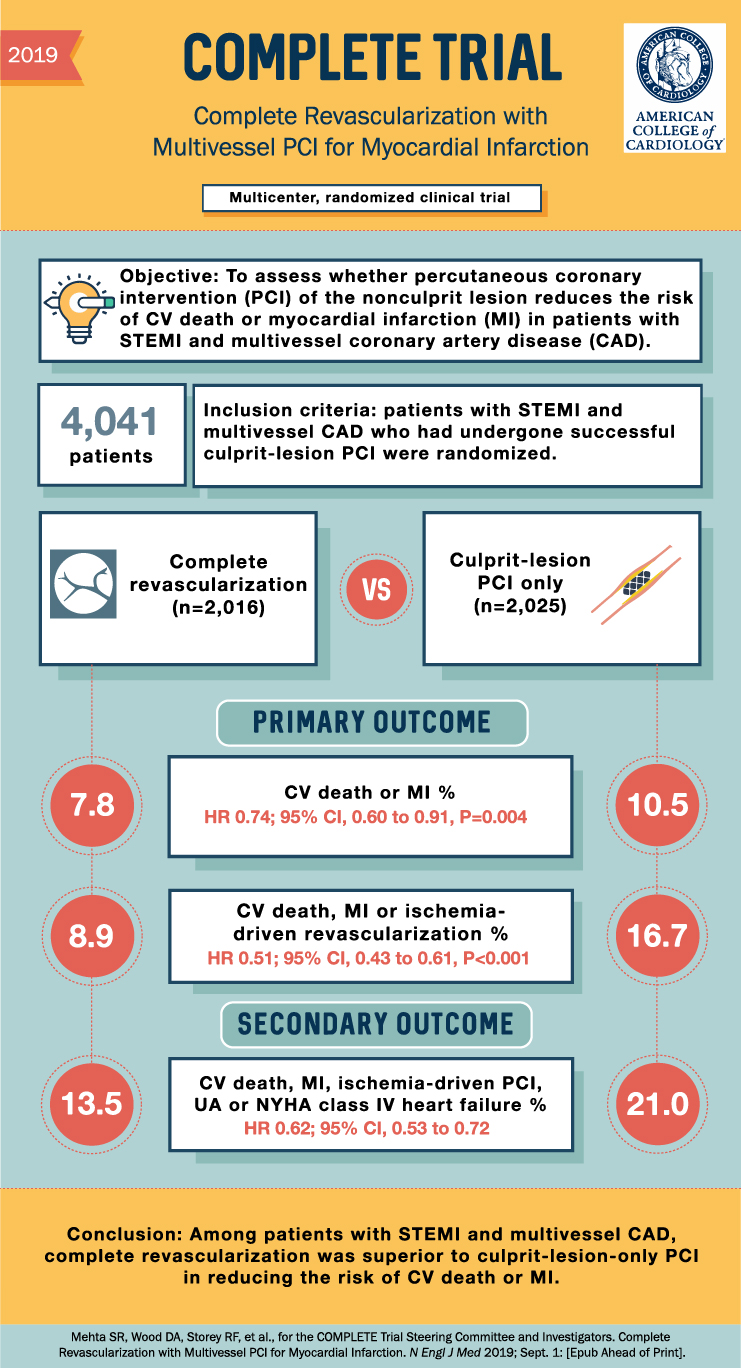
The objective of the COMPLETE trial was to assess whether percutaneous coronary intervention of nonculprit lesions reduces the risk of:
Cardiovascular death or myocardial infarction
in patients with:
STEMI and multivessel coronary artery disease
Study Design
The COMPLETE trial was a:
Multicenter, randomized clinical trial
A total of 4,041 patients were enrolled.
Patients had STEMI and multivessel coronary artery disease and had already undergone successful PCI of the culprit lesion.
They were then randomized to one of two strategies:
- Complete revascularization
Nonculprit lesions were also treated with PCI
n = 2,016 - Culprit-lesion PCI only
Only the artery responsible for the STEMI was treated
n = 2,025
Primary Outcome
The main outcome was the composite of:
Cardiovascular death or myocardial infarction
Results:
Complete revascularization: 7.8%
Culprit-lesion-only PCI: 10.5%
This represented a significant reduction in risk:
HR 0.74; 95% CI, 0.60 to 0.91; P = 0.004
This means that complete revascularization reduced the risk of cardiovascular death or myocardial infarction compared with culprit-lesion-only PCI.
Additional Primary Outcome
The trial also looked at the composite of:
Cardiovascular death, myocardial infarction, or ischemia-driven revascularization
Results:
Complete revascularization: 8.9%
Culprit-lesion-only PCI: 16.7%
Risk reduction:
HR 0.51; 95% CI, 0.43 to 0.61; P < 0.001
This was a large reduction, mainly driven by fewer ischemia-driven revascularization events in the complete revascularization group.
Secondary Outcome
A broader secondary outcome included:
Cardiovascular death, myocardial infarction, ischemia-driven PCI, unstable angina, or NYHA class IV heart failure
Results:
Complete revascularization: 13.5%
Culprit-lesion-only PCI: 21.0%
Risk reduction:
HR 0.62; 95% CI, 0.53 to 0.72
Again, complete revascularization was superior to treating only the culprit lesion.
Why the COMPLETE Trial Matters
The COMPLETE trial helped clarify the management of STEMI patients with multivessel coronary artery disease.
The trial showed that once the culprit lesion has been successfully treated, addressing significant nonculprit coronary lesions can reduce future cardiovascular events.
This is clinically important because multivessel disease is common in patients with STEMI. The COMPLETE trial supports a more comprehensive revascularization strategy rather than simply stopping after the culprit artery is opened.
Clinical Takeaway
For patients with STEMI and multivessel coronary artery disease, the COMPLETE trial showed that complete revascularization is superior to culprit-lesion-only PCI.
The benefit was seen in reduction of:
- Cardiovascular death or myocardial infarction
- Cardiovascular death, MI, or ischemia-driven revascularization
- Broader adverse cardiovascular outcomes including unstable angina and heart failure
Conclusion
The COMPLETE trial demonstrated that among patients with STEMI and multivessel coronary artery disease, complete revascularization reduced major cardiovascular events compared with culprit-lesion-only PCI.
In simple terms: after treating the culprit artery in STEMI, fixing the important nonculprit lesions as part of a complete revascularization strategy leads to better outcomes than leaving them alone.