Introduction
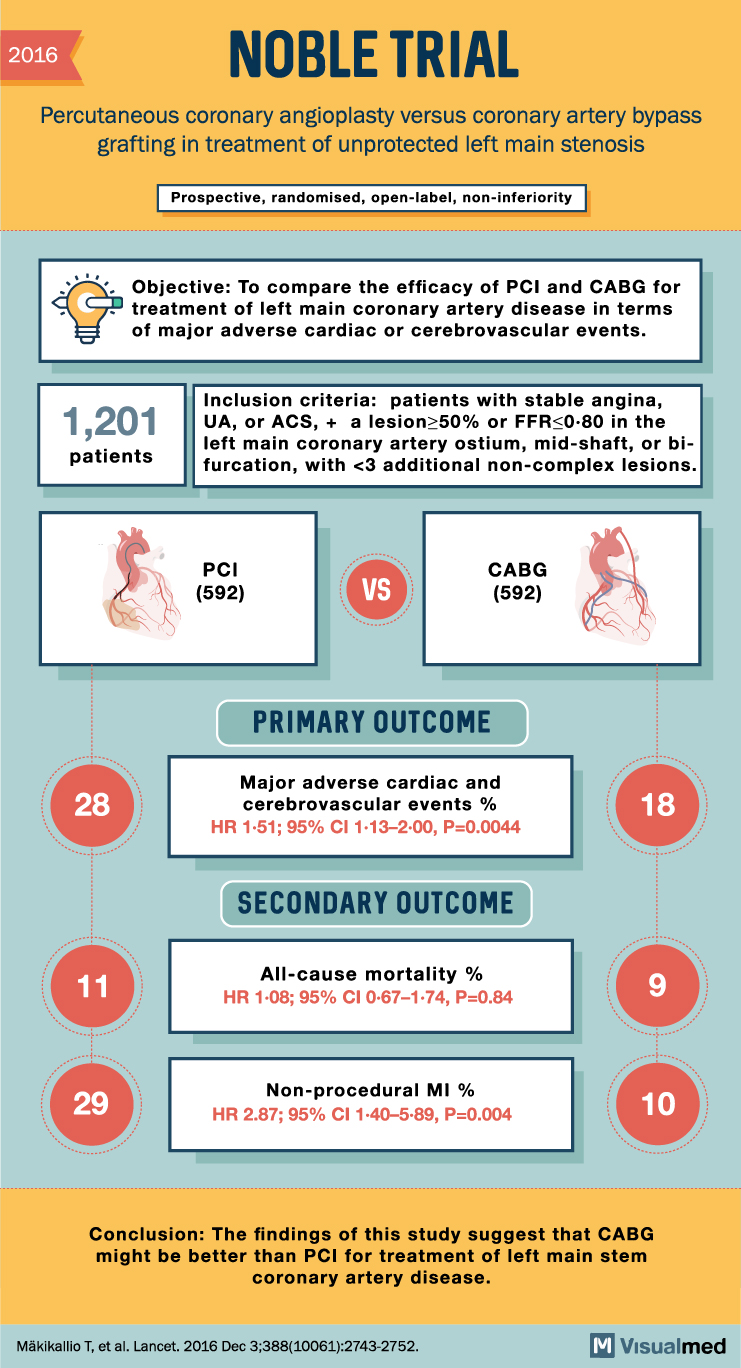
The NOBLE trial was an important randomized clinical trial comparing percutaneous coronary intervention (PCI) with coronary artery bypass grafting (CABG) in patients with unprotected left main coronary artery disease.
Left main coronary artery disease is clinically important because the left main artery supplies a large portion of the myocardium. Revascularization is usually required, but the best strategy — PCI or CABG — has been debated for years.
The NOBLE trial helped clarify this question by comparing PCI and CABG in patients with left main stem coronary artery disease.
Background
Historically, CABG has been considered the standard treatment for significant left main disease because it provides durable revascularization and bypasses complex proximal coronary lesions.
However, advances in PCI, including improved stent technology and procedural techniques, made PCI a potential alternative for selected patients.
The NOBLE trial was designed to test whether PCI was non-inferior to CABG for major adverse cardiac or cerebrovascular outcomes.
Study Design
The NOBLE trial was a:
Prospective, randomized, open-label, non-inferiority trial
A total of 1,201 patients were included.
Patients were randomized to:
PCI: 592 patients
CABG: 592 patients
The trial enrolled patients with unprotected left main coronary artery stenosis who were considered suitable for either PCI or CABG.
Inclusion Criteria
Patients were eligible if they had left main coronary artery disease with:
stenosis greater than 50%, or
fractional flow reserve FFR ≤0.80
Patients could have stable angina, unstable angina, or acute coronary syndrome.
The left main disease could involve the ostium, mid-shaft, or bifurcation, with fewer than three additional non-complex lesions.
Primary Outcome
The primary outcome was major adverse cardiac and cerebrovascular events.
This occurred in:
28% of patients in the PCI group
18% of patients in the CABG group
The hazard ratio was:
HR 1.51; 95% CI, 1.13 to 2.00; P=0.0044
This result favored CABG.
Secondary Outcomes
All-cause mortality
All-cause mortality occurred in:
11% of patients in the PCI group
9% of patients in the CABG group
The hazard ratio was:
HR 1.08; 95% CI, 0.67 to 1.74; P=0.84
There was no statistically significant difference in all-cause mortality between PCI and CABG.
Non-procedural myocardial infarction
Non-procedural myocardial infarction occurred in:
29% of patients in the PCI group
10% of patients in the CABG group
The hazard ratio was:
HR 2.87; 95% CI, 1.40 to 5.89; P=0.004
This strongly favored CABG.
Main Findings of the NOBLE Trial
The NOBLE trial found that PCI was associated with a higher rate of major adverse cardiac and cerebrovascular events compared with CABG in patients with unprotected left main coronary artery disease.
The difference was mainly driven by higher rates of non-procedural myocardial infarction and repeat adverse cardiovascular events after PCI.
Mortality alone was not significantly different between the two groups, but the overall composite outcome favored CABG.
Clinical Importance
The NOBLE trial is important because it challenged the idea that PCI could routinely replace CABG for left main coronary artery disease.
The findings suggest that while PCI may be appropriate for selected patients, CABG remains the more durable strategy for many patients with left main disease.
This is especially relevant when the goal is to reduce long-term myocardial infarction and major adverse cardiac or cerebrovascular events.
NOBLE Trial vs EXCEL Trial
The NOBLE trial is often discussed alongside the EXCEL trial, another major study comparing PCI and CABG for left main coronary artery disease.
While EXCEL suggested broadly similar rates of death, stroke, or myocardial infarction in selected patients, NOBLE showed worse outcomes with PCI for the composite endpoint.
Together, these trials highlight that treatment decisions for left main coronary artery disease should be individualized and ideally made by a heart team considering anatomy, surgical risk, SYNTAX score, patient preference, and long-term durability.
Practical Takeaway
The NOBLE trial supports CABG as the preferred revascularization strategy for many patients with unprotected left main coronary artery disease.
PCI remains an option in selected patients, especially when surgical risk is high or anatomy is favorable, but the NOBLE trial showed a higher risk of major adverse cardiac and cerebrovascular events with PCI compared with CABG.
Conclusion
The NOBLE trial demonstrated that CABG may provide better long-term outcomes than PCI for patients with unprotected left main coronary artery disease.
Although mortality was similar between groups, PCI was associated with more major adverse cardiac and cerebrovascular events and more non-procedural myocardial infarction.
For patients with left main coronary artery disease, the NOBLE trial remains a key study supporting careful heart-team decision-making between PCI and CABG.
Reference
Mäkikallio T, et al. Percutaneous coronary angioplasty versus coronary artery bypass grafting in treatment of unprotected left main stenosis. Lancet. 2016;388:2743-2752.