The COURAGE trial was one of the most important landmark cardiology trials because it challenged the routine use of percutaneous coronary intervention, or PCI, in patients with stable coronary artery disease. Before COURAGE, many patients with stable coronary blockages underwent PCI with the expectation that opening the artery would reduce future heart attacks or death. The trial showed that when patients receive strong guideline-directed medical therapy, adding PCI does not significantly reduce death or nonfatal myocardial infarction compared with medical therapy alone.
Background: Why Was the COURAGE Trial Important?
PCI is clearly beneficial in acute coronary syndromes, especially in patients presenting with ST-elevation myocardial infarction or high-risk unstable presentations. However, the benefit of PCI in stable coronary artery disease was less clear. The key clinical question was whether PCI should be used early in stable patients to prevent death or myocardial infarction, or whether aggressive medical therapy should be the first-line strategy.
The COURAGE trial was designed to answer this question directly.
Study Design
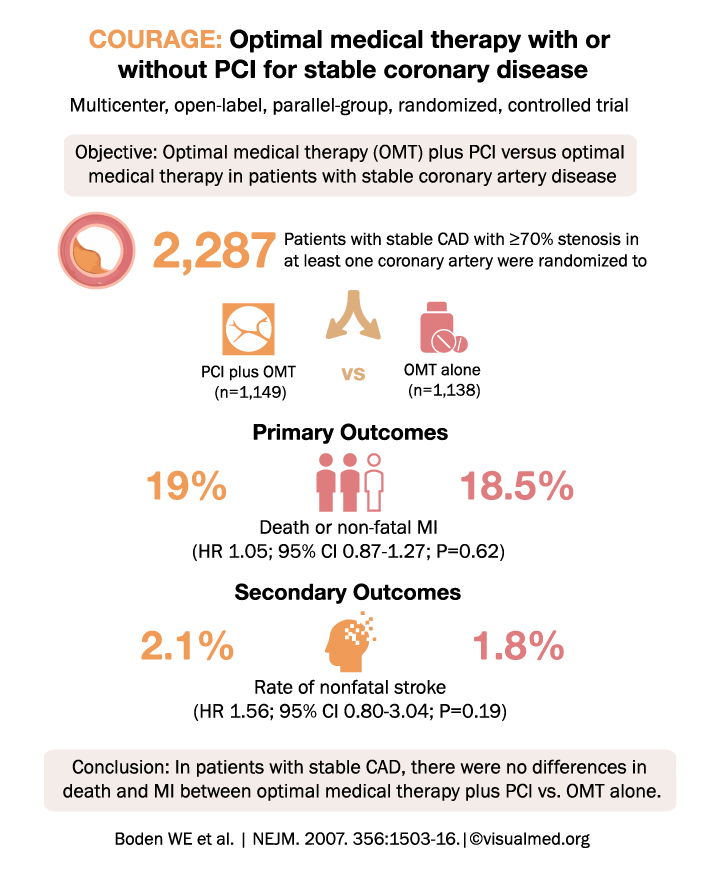
The COURAGE trial was a multicenter, open-label, randomized controlled trial published in the New England Journal of Medicine in 2007. It enrolled 2,287 patients with stable coronary artery disease and significant coronary stenosis. Patients were randomized to one of two treatment strategies:
- PCI plus optimal medical therapy
- Optimal medical therapy alone
Optimal medical therapy included antianginal therapy, antiplatelet therapy, lipid-lowering therapy, blood pressure control, lifestyle modification, and risk-factor management.
Primary Outcome
The primary outcome of the COURAGE trial was a composite of:
Death from any cause or nonfatal myocardial infarction
The results showed:
- PCI plus optimal medical therapy: 19.0%
- Optimal medical therapy alone: 18.5%
There was no statistically significant difference between the two groups. The hazard ratio was 1.05, with a 95% confidence interval of 0.87 to 1.27 and a P value of 0.62.
Secondary Outcomes
One of the secondary outcomes was nonfatal stroke:
- PCI plus optimal medical therapy: 2.1%
- Optimal medical therapy alone: 1.8%
This difference was also not statistically significant.
Main Finding of the COURAGE Trial
The major message of the COURAGE trial was simple:
In patients with stable coronary artery disease, an initial strategy of PCI added to optimal medical therapy did not reduce the risk of death or nonfatal myocardial infarction compared with optimal medical therapy alone.
This finding changed how clinicians approached stable coronary disease. Instead of automatically sending stable patients for PCI, the COURAGE trial supported a strategy of starting with aggressive medical therapy and reserving PCI mainly for patients with persistent symptoms despite medical treatment.
Clinical Interpretation
The COURAGE trial does not mean PCI has no role in stable coronary artery disease. PCI can still be very useful for symptom relief, especially in patients with angina that persists despite good medical therapy. However, the trial showed that PCI should not be expected to reduce death or myocardial infarction in stable patients when compared with optimal medical therapy.
In practical terms, the COURAGE trial reinforced the importance of:
- Intensive lipid lowering
- Blood pressure control
- Antiplatelet therapy when appropriate
- Smoking cessation
- Exercise and diet modification
- Antianginal therapy
- Careful patient selection for PCI
Why the COURAGE Trial Still Matters
The COURAGE trial remains highly relevant because stable coronary artery disease is extremely common. Many patients and clinicians assume that fixing a coronary blockage automatically prevents future heart attacks. COURAGE helped clarify that stable coronary disease is often a systemic atherosclerotic process, and that aggressive medical therapy is central to improving outcomes.
The trial also laid the foundation for later studies, including ISCHEMIA, which further examined invasive versus conservative strategies in stable ischemic heart disease.
Conclusion
The COURAGE trial showed that in patients with stable coronary artery disease, adding PCI to optimal medical therapy did not reduce death or nonfatal myocardial infarction compared with optimal medical therapy alone. PCI remains important for symptom relief in selected patients, but the COURAGE trial strongly supports optimal medical therapy as the initial foundation of care for stable coronary artery disease.