What is EKG axis?
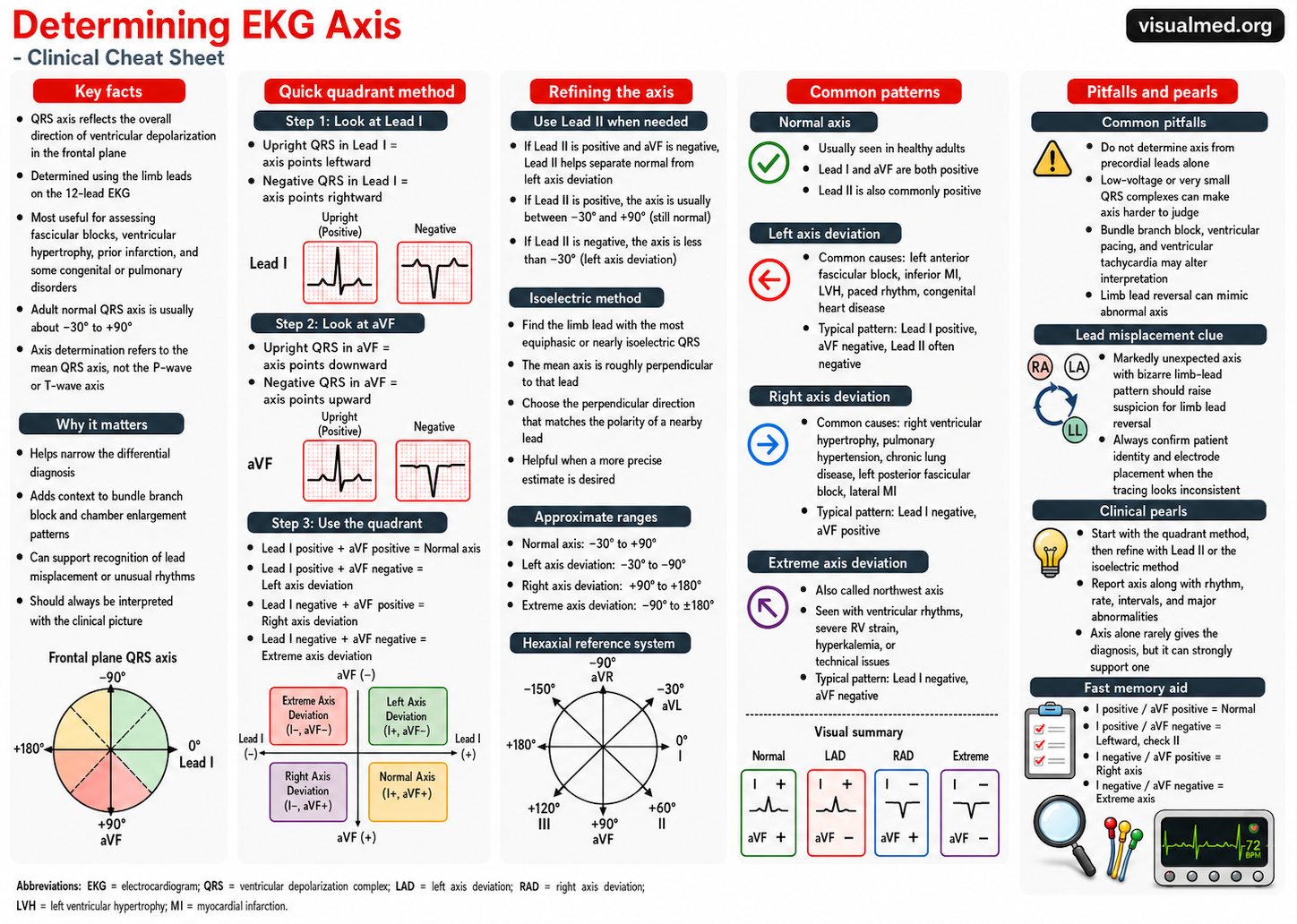
The EKG axis describes the overall direction of ventricular depolarization in the frontal plane. In practical terms, when clinicians talk about “axis,” they are usually referring to the mean QRS axis.
A normal QRS axis generally points downward and to the left, because the left ventricle contributes most of the ventricular electrical force. A normal adult QRS axis is commonly defined as between -30° and +90°. Axis deviation can suggest conduction disease, chamber enlargement, myocardial infarction, ventricular rhythms, or other structural/electrical abnormalities. LITFL, StatPearls
The fastest method: Lead I and aVF
The quickest bedside method uses two limb leads:
Lead I tells you whether the electrical vector is moving leftward or rightward.
aVF tells you whether the electrical vector is moving downward or upward.
Look at the QRS complex in each lead and decide whether it is mostly positive or mostly negative.
| Lead I | aVF | Axis Pattern |
|---|---|---|
| Positive | Positive | Normal axis |
| Positive | Negative | Possible left axis deviation |
| Negative | Positive | Right axis deviation |
| Negative | Negative | Extreme axis deviation |
This is often called the quadrant method.
Step 1: Look at Lead I
If the QRS complex in Lead I is mostly upright, the axis is generally directed toward the patient’s left side.
Lead I positive = leftward direction
If the QRS complex in Lead I is mostly negative, the axis is generally directed away from the left side and toward the right.
Lead I negative = rightward direction
Step 2: Look at aVF
If the QRS complex in aVF is mostly upright, the axis is directed inferiorly.
aVF positive = downward direction
If the QRS complex in aVF is mostly negative, the axis is directed superiorly.
aVF negative = upward direction
Normal axis
A normal axis occurs when:
Lead I is positive
aVF is positive
This places the QRS axis between approximately 0° and +90°, which falls within the normal adult range. LITFL
Common interpretation:
Lead I positive + aVF positive = normal axis
Left axis deviation
Left axis deviation is usually defined as a QRS axis less than -30°. LITFL
The typical screening pattern is:
Lead I positive
aVF negative
However, this pattern alone can include both true left axis deviation and a borderline/physiologic axis between 0° and -30°. That is why Lead II is helpful.
If Lead I is positive and aVF is negative, check Lead II:
Lead II positive: axis may still be normal/borderline
Lead II negative: left axis deviation is more likely
Common causes of left axis deviation include:
Left anterior fascicular block
Inferior myocardial infarction
Left ventricular hypertrophy
Left bundle branch block
Ventricular rhythms
Normal variant in some patients
Right axis deviation
Right axis deviation is usually defined as a QRS axis greater than +90°. LITFL
The classic pattern is:
Lead I negative
aVF positive
Common causes include:
Right ventricular hypertrophy
Right bundle branch block
Left posterior fascicular block
Pulmonary hypertension
Pulmonary embolism or acute right heart strain
Lateral myocardial infarction
Ventricular rhythms
Dextrocardia
Normal variant, especially in young or thin adults
Extreme axis deviation
Extreme axis deviation, also called northwest axis, occurs when the QRS axis is between approximately -90° and 180°. LITFL
The pattern is:
Lead I negative
aVF negative
This is an abnormal axis pattern and should raise concern for unusual ventricular activation.
Possible causes include:
Ventricular tachycardia
Ventricular paced rhythm
Severe conduction disease
Hyperkalemia
Certain congenital heart disease patterns
Technical error such as limb lead reversal
Always make sure the limb leads are placed correctly before over-interpreting an extreme axis.
The Lead II check
Lead II helps clarify the gray zone between normal axis and left axis deviation.
If:
Lead I is positive
aVF is negative
Then look at Lead II.
If Lead II is still positive, the axis is usually between -30° and 0°, which is often considered borderline or still within normal range.
If Lead II is negative, the axis is more negative than -30°, supporting left axis deviation.
Practical clinical approach
Use this simple sequence:
- Look at Lead I.
- Look at aVF.
- Classify the quadrant.
- If Lead I is positive and aVF is negative, check Lead II.
- Confirm the axis fits the clinical picture.
- Exclude lead misplacement if the axis looks strange.
Common mistakes
One common mistake is calling left axis deviation whenever Lead I is positive and aVF is negative. That pattern only tells you the axis is somewhere between 0° and -90°. Lead II helps decide whether it is truly beyond -30°.
Another mistake is using precordial leads to determine frontal plane axis. Axis determination is based on the limb leads.
A third mistake is ignoring lead reversal. If the axis is bizarre, the P waves look unusual, or Lead I is unexpectedly inverted, check for limb lead misplacement.
Clinical takeaway
EKG axis is easiest when you reduce it to two leads:
Lead I = left vs right
aVF = down vs up
The core patterns are:
Lead I positive + aVF positive = normal axis
Lead I positive + aVF negative = possible LAD; check Lead II
Lead I negative + aVF positive = RAD
Lead I negative + aVF negative = extreme axis
This simple method is fast, reliable, and clinically useful for everyday EKG interpretation.
References
- LITFL. ECG Axis Interpretation. https://litfl.com/ecg-axis-interpretation/
- StatPearls. Electrical Right and Left Axis Deviation. NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK470532/