Supraventricular tachycardia, commonly abbreviated as SVT, refers to a group of fast heart rhythms that arise above the ventricles. These rhythms usually originate from the atria, the AV node, or an accessory pathway involving tissue outside the normal conduction system.
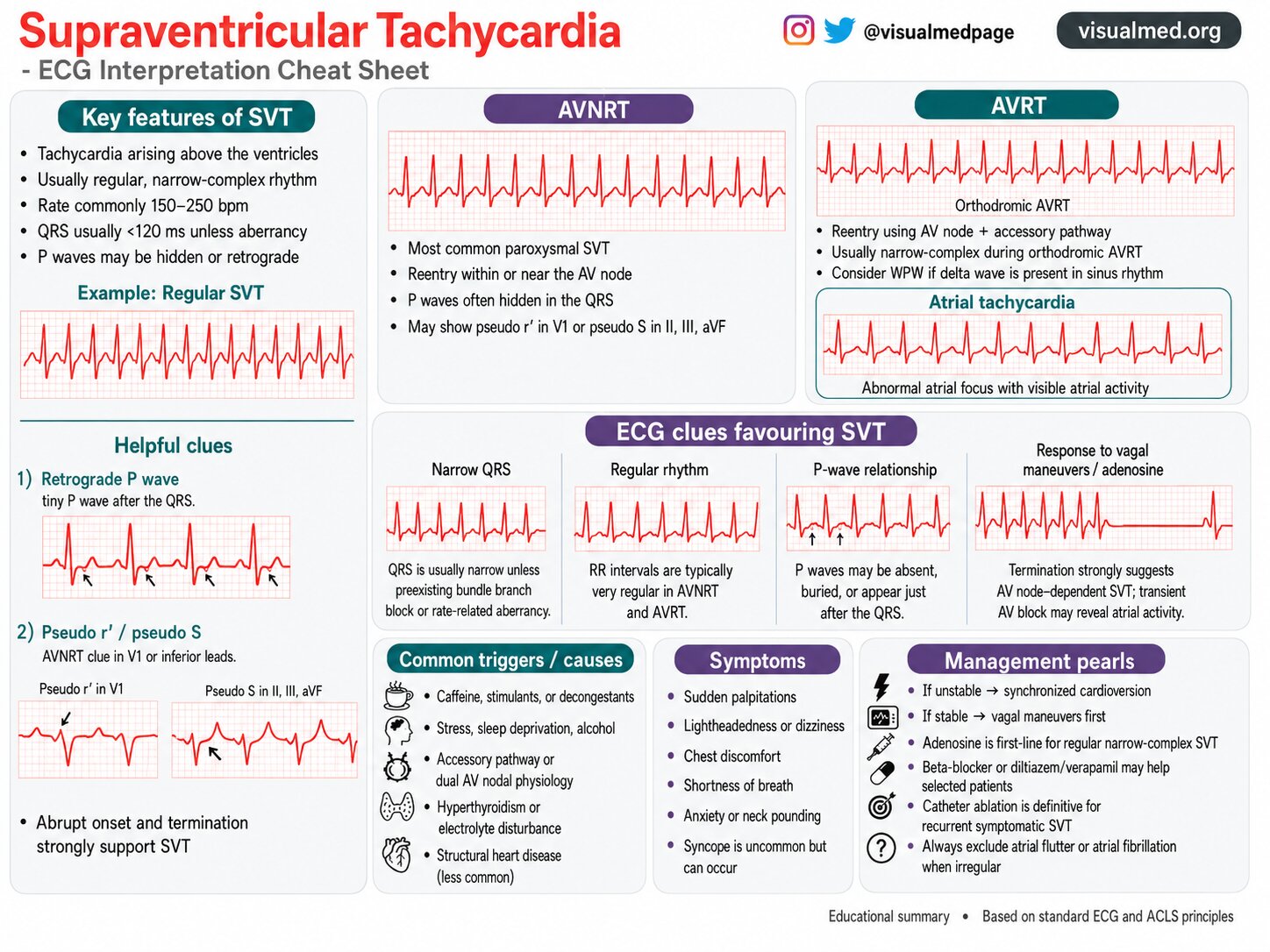
On ECG, SVT most often appears as a regular narrow-complex tachycardia with a rapid ventricular rate, commonly between 150 and 250 beats per minute. Although many cases are not immediately life-threatening, SVT can cause significant symptoms and may require urgent treatment when associated with hemodynamic instability.
This ECG cheat sheet reviews the key features of SVT, common subtypes, helpful diagnostic clues, triggers, symptoms, and practical management pearls.
What Is SVT?
SVT is an umbrella term for tachyarrhythmias that originate above the ventricles. Because ventricular activation usually travels through the His-Purkinje system, the QRS complex is typically narrow, usually less than 120 ms.
However, SVT can occasionally appear as a wide-complex rhythm if there is preexisting bundle branch block, rate-related aberrancy, or conduction over an accessory pathway.
Common forms of SVT include:
- AV nodal reentrant tachycardia
- Atrioventricular reentrant tachycardia
- Atrial tachycardia
Atrial flutter and atrial fibrillation are also supraventricular rhythms, but they are often discussed separately because their ECG patterns and management considerations differ.
Key ECG Features of SVT
Classic SVT usually has several recognizable ECG features:
- Tachycardia arising above the ventricles
- Usually regular rhythm
- Usually narrow QRS complex
- Rate commonly 150–250 bpm
- P waves may be hidden, retrograde, or difficult to identify
The most typical ECG appearance is a rapid, regular, narrow-complex tachycardia with no clearly visible P waves.
When the rhythm begins and ends abruptly, this strongly supports a reentrant mechanism such as AVNRT or AVRT.
AVNRT: The Most Common Paroxysmal SVT
AV nodal reentrant tachycardia, or AVNRT, is the most common type of paroxysmal SVT.
In AVNRT, the tachycardia circuit occurs within or near the AV node. Because atrial and ventricular activation occur almost simultaneously, P waves are often hidden inside the QRS complex.
ECG clues for AVNRT
AVNRT may show:
- Regular narrow-complex tachycardia
- P waves hidden in the QRS
- Pseudo r′ wave in V1
- Pseudo S waves in inferior leads II, III, and aVF
These subtle findings can help distinguish AVNRT from other narrow-complex tachycardias.
AVRT: SVT Using an Accessory Pathway
Atrioventricular reentrant tachycardia, or AVRT, involves a reentry circuit that uses both the AV node and an accessory pathway.
The most common form is orthodromic AVRT, where conduction travels down the AV node and back up the accessory pathway. Because ventricular activation still occurs through the normal conduction system, the QRS is usually narrow.
ECG clues for AVRT
AVRT may show:
- Regular narrow-complex tachycardia
- Retrograde P waves after the QRS
- History or ECG evidence of Wolff-Parkinson-White pattern
- Delta wave during sinus rhythm if preexcitation is present
When a patient has a delta wave on baseline ECG, an accessory pathway should be considered.
Atrial Tachycardia
Atrial tachycardia occurs when an abnormal atrial focus drives the rhythm.
Unlike AVNRT or AVRT, atrial tachycardia does not require the AV node as part of the reentry circuit. This means adenosine may transiently slow AV conduction and reveal atrial activity without necessarily terminating the rhythm.
ECG clues for atrial tachycardia
Atrial tachycardia may show:
- Visible abnormal P waves
- Atrial activity before each QRS
- Narrow QRS unless aberrancy is present
- Variable response to AV nodal blocking maneuvers
Recognizing atrial activity is important because management may differ from AV node–dependent SVT.
Helpful ECG Clues Favoring SVT
When evaluating a tachycardia, several ECG features can help support SVT.
1. Narrow QRS Complex
SVT usually produces a narrow QRS because ventricular activation occurs through the normal His-Purkinje system.
A narrow QRS strongly favors a supraventricular origin, although it does not identify the exact SVT mechanism.
2. Regular Rhythm
AVNRT and AVRT are usually very regular. The RR intervals are typically consistent from beat to beat.
An irregular rhythm should raise suspicion for atrial fibrillation, atrial flutter with variable conduction, or multifocal atrial tachycardia rather than classic AVNRT or AVRT.
3. P-Wave Relationship
P waves in SVT may be:
- Hidden inside the QRS
- Seen just after the QRS
- Retrograde in appearance
- Visible before the QRS in atrial tachycardia
The relationship between P waves and QRS complexes can help determine whether the rhythm is AVNRT, AVRT, or atrial tachycardia.
4. Response to Vagal Maneuvers or Adenosine
AV node–dependent SVTs often respond to vagal maneuvers or adenosine.
If the rhythm terminates abruptly after vagal maneuvers or adenosine, AVNRT or AVRT becomes more likely.
If adenosine causes transient AV block but the atrial rhythm continues, this may reveal atrial flutter or atrial tachycardia.
Retrograde P Waves
Retrograde P waves occur when atrial activation travels backward from the AV node or accessory pathway into the atria.
On ECG, they may appear just after the QRS complex. Depending on the lead, they may be inverted.
This is a useful clue in AVNRT and AVRT, especially when the P wave is small and easy to miss.
Pseudo r′ and Pseudo S Waves
In AVNRT, retrograde atrial activation may distort the terminal portion of the QRS complex.
This can create:
- A pseudo r′ wave in V1
- A pseudo S wave in inferior leads
These are subtle findings, but they can be very helpful when comparing the tachycardia ECG with the patient’s baseline ECG.
Common Triggers and Causes
SVT can occur in otherwise healthy hearts, but several triggers and underlying factors may contribute.
Common triggers include:
- Caffeine
- Stimulants
- Decongestants
- Stress
- Sleep deprivation
- Alcohol
- Electrolyte disturbance
- Hyperthyroidism
Underlying mechanisms may include:
- Dual AV nodal physiology
- Accessory pathway
- Atrial ectopic focus
- Structural heart disease, less commonly
Identifying triggers can help reduce recurrence in some patients.
Common Symptoms of SVT
SVT often presents suddenly. Patients may describe an abrupt onset of rapid heartbeat.
Common symptoms include:
- Sudden palpitations
- Lightheadedness
- Dizziness
- Chest discomfort
- Shortness of breath
- Anxiety
- Neck pounding
Syncope is less common but can occur, especially if the rhythm is very rapid or the patient has underlying cardiac disease.
Initial Management Pearls
Management depends on whether the patient is stable or unstable.
If the patient is unstable
If SVT is associated with hypotension, shock, altered mental status, ischemic chest discomfort, or acute heart failure, urgent synchronized cardioversion is generally required.
If the patient is stable
For stable regular narrow-complex SVT, initial management often includes:
- Vagal maneuvers
- Adenosine
- AV nodal blockers in selected patients
Beta-blockers, diltiazem, or verapamil may be considered in appropriate stable patients, depending on the clinical context and contraindications.
For recurrent symptomatic SVT, catheter ablation can be definitive therapy.
Important Pitfall: Do Not Miss Atrial Flutter or Atrial Fibrillation
Not every narrow-complex tachycardia is AVNRT or AVRT.
If the rhythm is irregular, always consider:
- Atrial fibrillation
- Atrial flutter with variable block
- Multifocal atrial tachycardia
Adenosine may help reveal atrial activity, but it should be used carefully and in the appropriate clinical setting.
Practical ECG Approach
When looking at a suspected SVT ECG, ask:
- Is the QRS narrow or wide?
- Is the rhythm regular or irregular?
- Are P waves visible?
- Are P waves before, within, or after the QRS?
- Is there abrupt onset and termination?
- Does the rhythm respond to vagal maneuvers or adenosine?
- Is there evidence of preexcitation on the baseline ECG?
This systematic approach can help narrow the differential diagnosis quickly.
Key Takeaway
SVT most commonly appears as a regular narrow-complex tachycardia with rapid rate and hidden or retrograde P waves.
The most common forms include AVNRT, AVRT, and atrial tachycardia. ECG clues such as narrow QRS, regular rhythm, P-wave relationship, pseudo r′ or pseudo S waves, and response to vagal maneuvers or adenosine can help identify the mechanism.
For unstable patients, synchronized cardioversion is the priority. For stable regular narrow-complex SVT, vagal maneuvers and adenosine are key early options.
Recognizing SVT quickly helps guide safe, effective treatment and prevents confusion with other tachyarrhythmias.