Year: 2010 Title: CURRENT-OASIS 7 Subtitle: Double-dose versus standard-dose clopidogrel and high-dose versus low-dose aspirin in individuals undergoing PCI for ACS Type of Trial: Double-blind, Randomized Factorial Trial
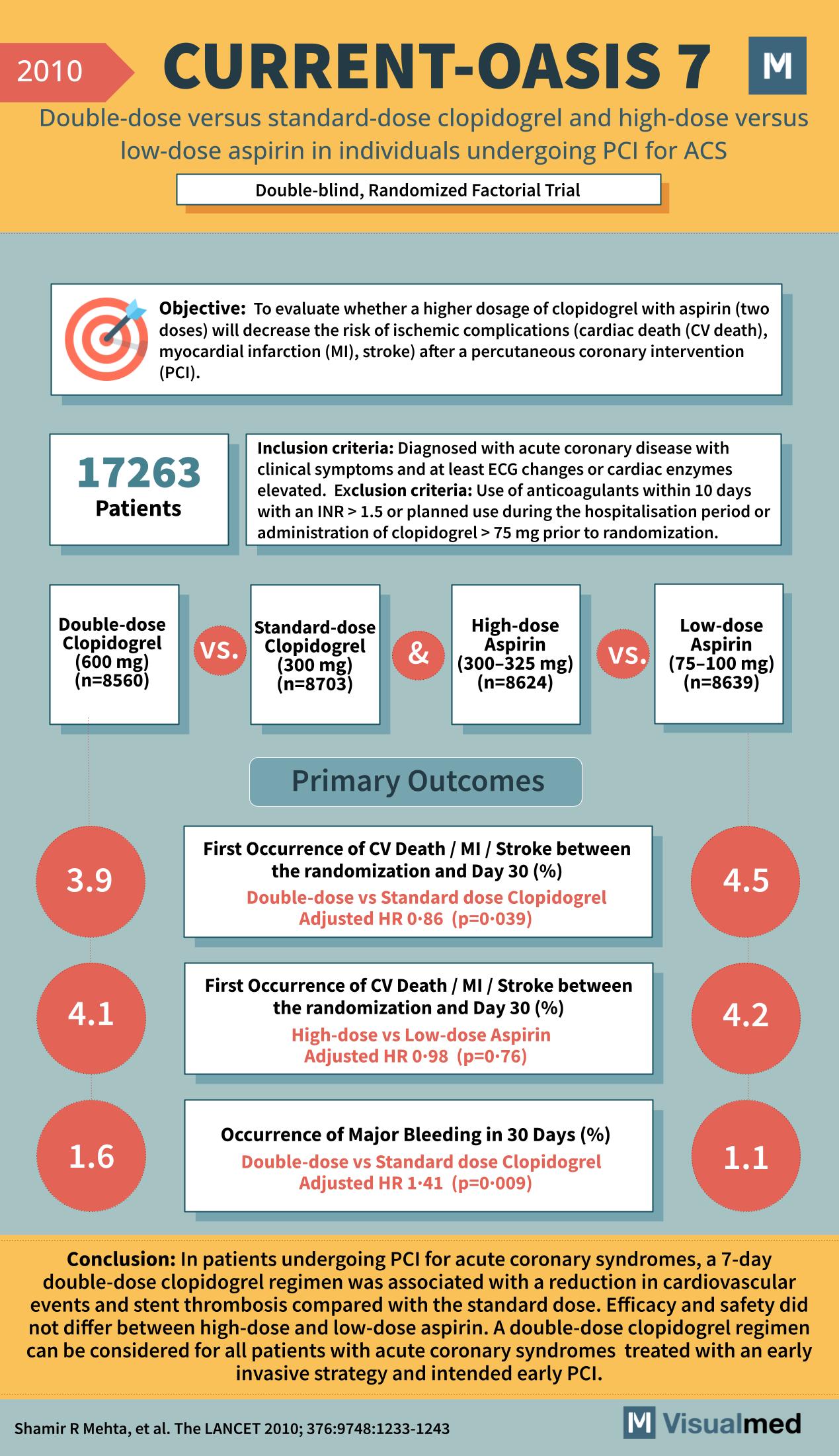
Objective: To evaluate whether a higher dosage of clopidogrel with aspirin (two doses) will decrease the risk of ischemic complications (cardiac death (CV death), myocardial infarction (MI), stroke) after a percutaneous coronary intervention (PCI).
Patients: 17,263
Inclusion Criteria: Diagnosed with acute coronary disease with clinical symptoms and at least ECG changes or cardiac enzymes elevated. Exclusion Criteria: Use of anticoagulants within 10 days with an INR > 1.5 or planned use during the hospitalization period or administration of clopidogrel > 75 mg prior to randomization.
Comparisons:
- Double-dose Clopidogrel (600 mg) (n=8560) vs. Standard-dose Clopidogrel (300 mg) (n=8703)
- High-dose Aspirin (300–325 mg) (n=8624) vs. Low-dose Aspirin (75–100 mg) (n=8639)
Primary Outcomes:
- First Occurrence of CV Death / MI / Stroke between the randomization and Day 30 (%)
- Double-dose vs Standard dose Clopidogrel: 3.9% (Adjusted HR 0.86, p=0.039)
- High-dose vs Low-dose Aspirin: 4.1% vs 4.2% (Adjusted HR 0.98, p=0.76)
- Occurrence of Major Bleeding in 30 Days (%)
- Double-dose vs Standard dose Clopidogrel: 1.6% vs 1.1% (Adjusted HR 1.41, p=0.009)
Conclusion: In patients undergoing PCI for acute coronary syndromes, a 7-day double-dose clopidogrel regimen was associated with a reduction in cardiovascular events and stent thrombosis compared with the standard dose. Efficacy and safety did not differ between high-dose and low-dose aspirin. A double-dose clopidogrel regimen can be considered for all patients with acute coronary syndromes treated with an early invasive strategy and intended early PCI.
Reference: Shamir R Mehta, et al. The Lancet 2010; 376:9748:1233-1243